
作者/講者: 林廷遠 醫師
筆記與整理: 陳羿方 醫師
校稿: Ian YC Chen, MD
上次校閱: 2018/09/29
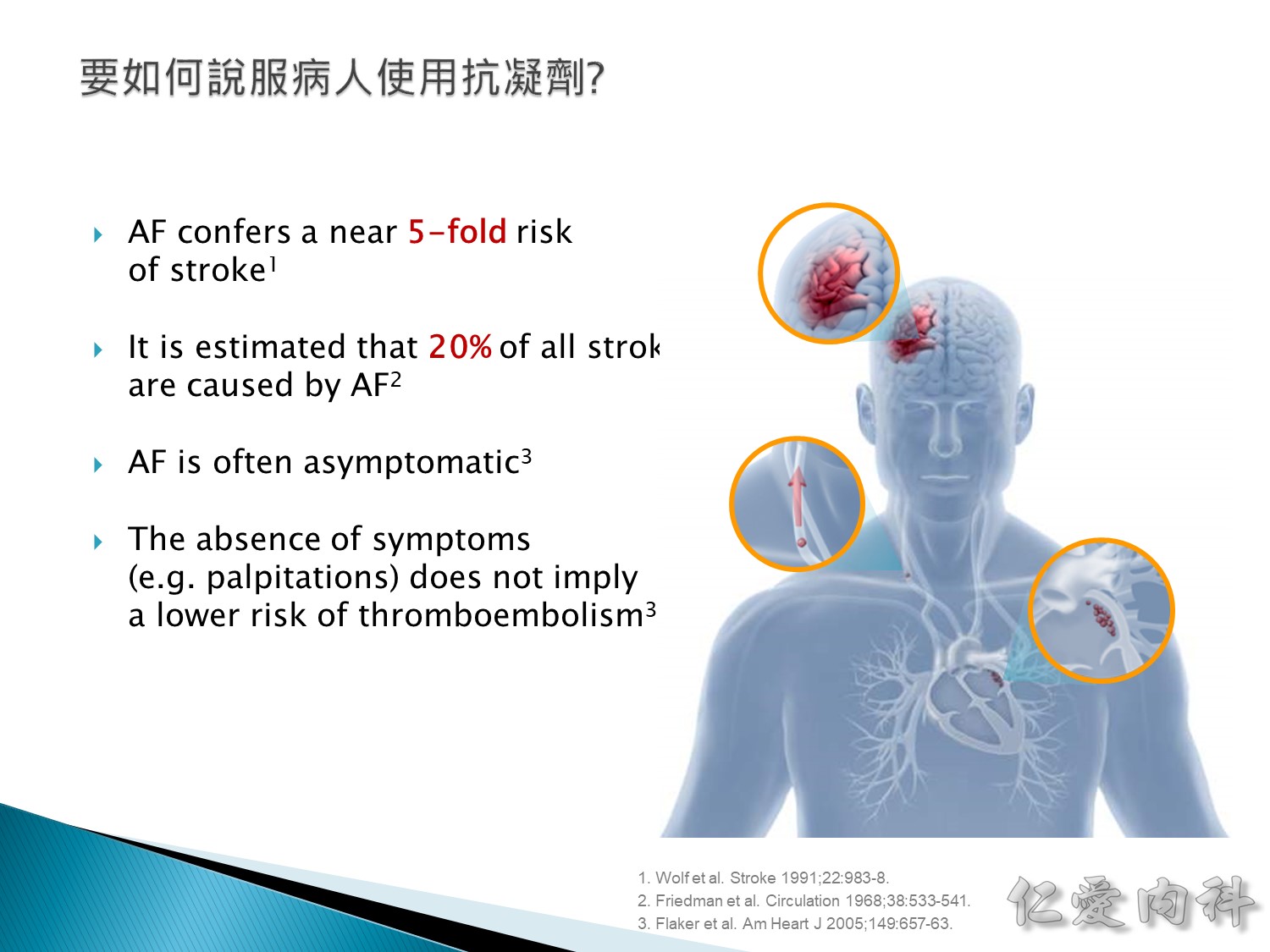
The impact of non-rheumatic AF, among other cardiac diseases, on stroke incidence was examined in 5,070 participants in the Framingham Study after
34 years of follow-up.1 Compared with subjects free of cardiovascular disease including AF, there was a near fivefold excess of stroke when AF was present (p<0.001). In persons with coronary heart disease or cardiac failure, AF doubled the stroke risk in men and trebled the risk in women.1The frequencies of prior cardiovascular abnormalities were compared
in 117 stroke patients and 234 matched control subjects.2 All were residents
of a retirement community and followed in the local medical clinic before the strokes occurred. There was a stronger association of stroke with AF than with other cardiac abnormalities. Not only was the frequency of AF about six times greater among stroke cases than controls, but about one fifth of all strokes observed occurred among persons with AF.2The Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) study showed that AF was often asymptomatic in men. However, the absence
of symptoms did not confer a more favorable prognosis.3
Abbreviations
AF: Atrial fibrillation
References
1. Wolf PA et al. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke 1991;22:983-8.
2. Friedman et al. Relationship of stroke to other cardiovascular disease. Circulation 1968;38:533-41.
3. Flaker GC et al; AFFIRM Investigators. Asymptomatic atrial fibrillation: demographic features and prognostic information from the Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) study. Am Heart J 2005;149:657-63.
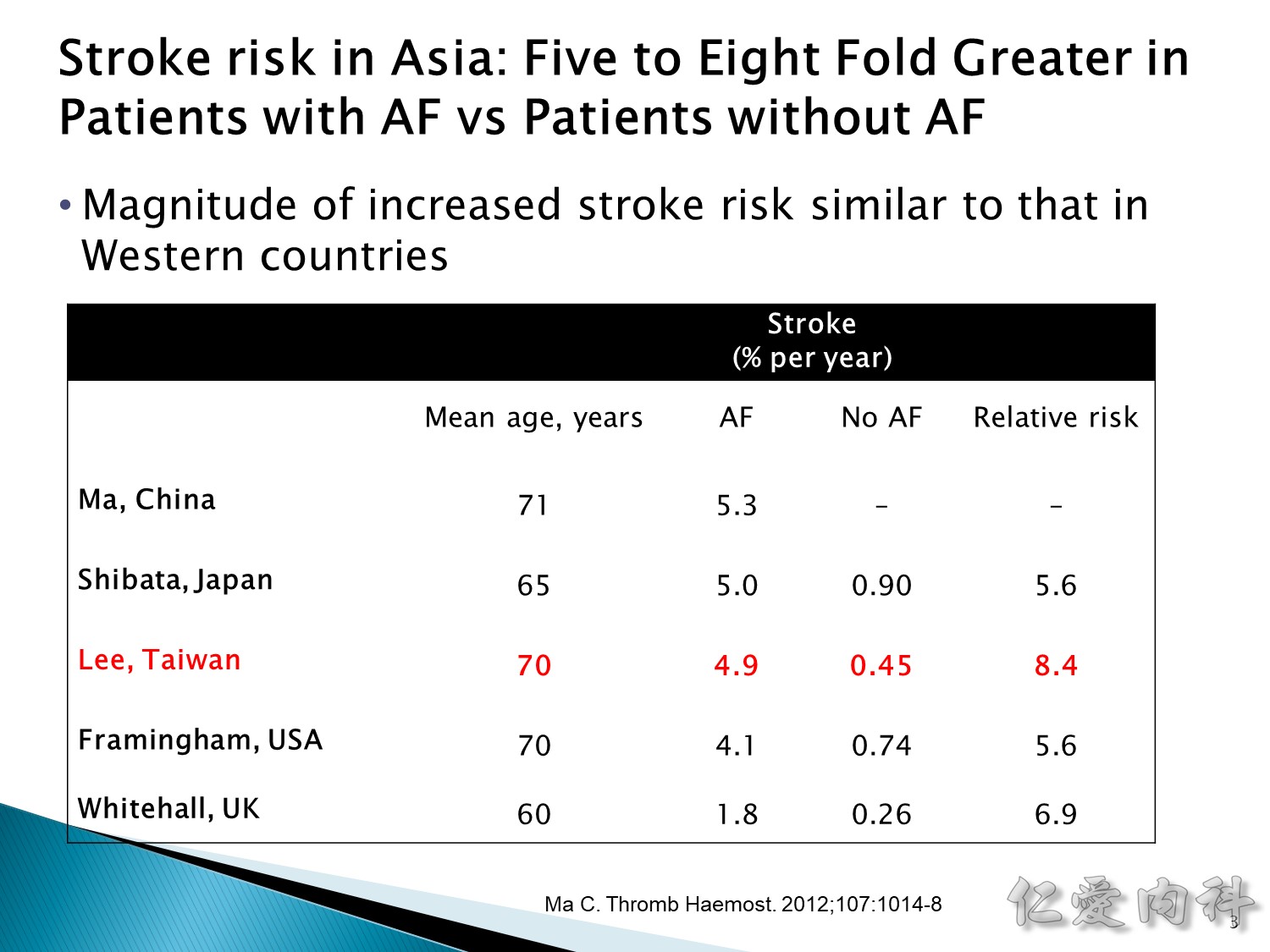
心房顫動發生中風的流行病學研究:
不論人種,罹患 AF 的病患其中風發生率約為沒有 AF 的 5~8 倍。
台灣研究顯示發生率兩者差為 8.4 倍。
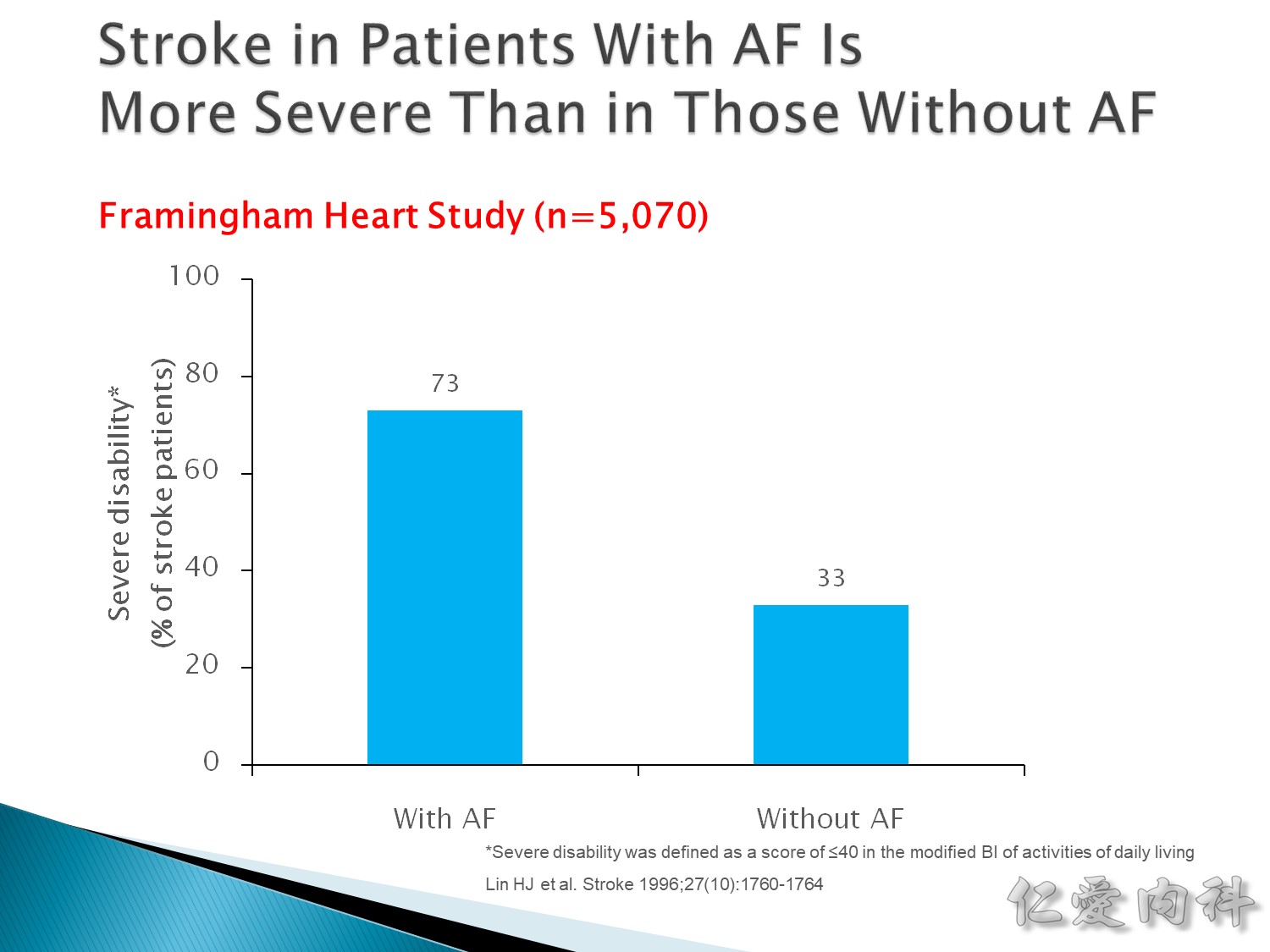
AF 的中風造成的危害比不是 AF 造成的危害來的更大。
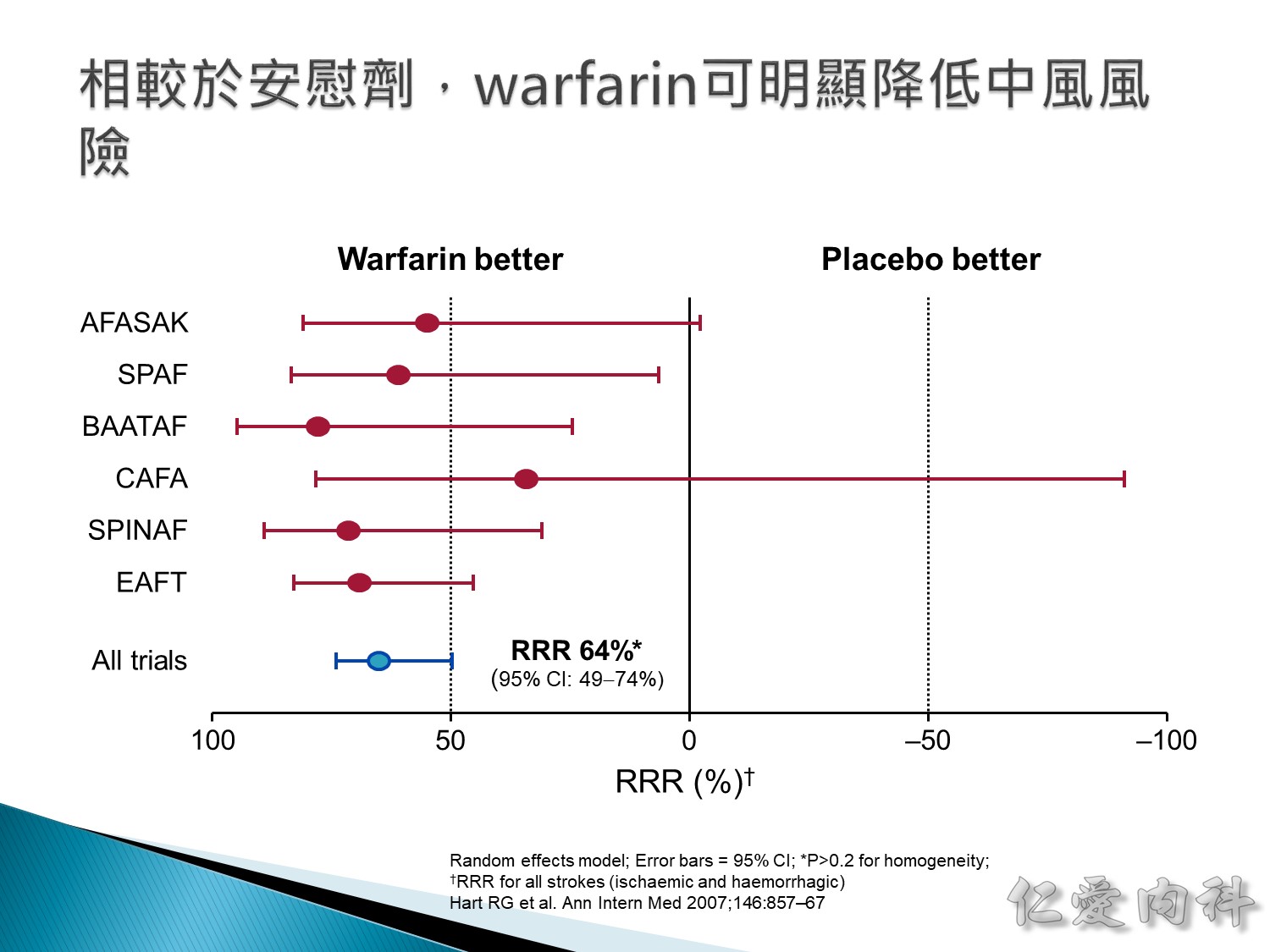
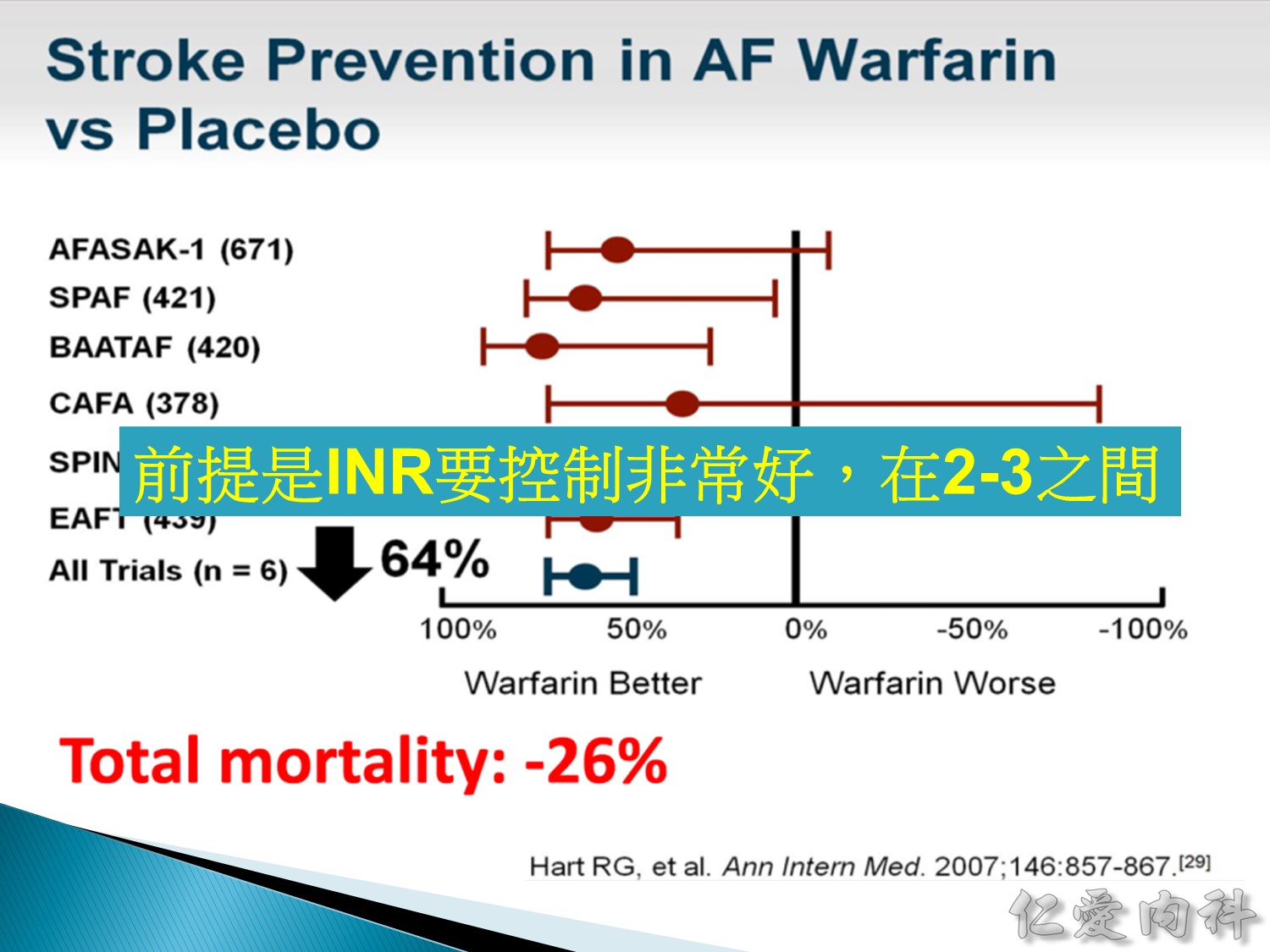
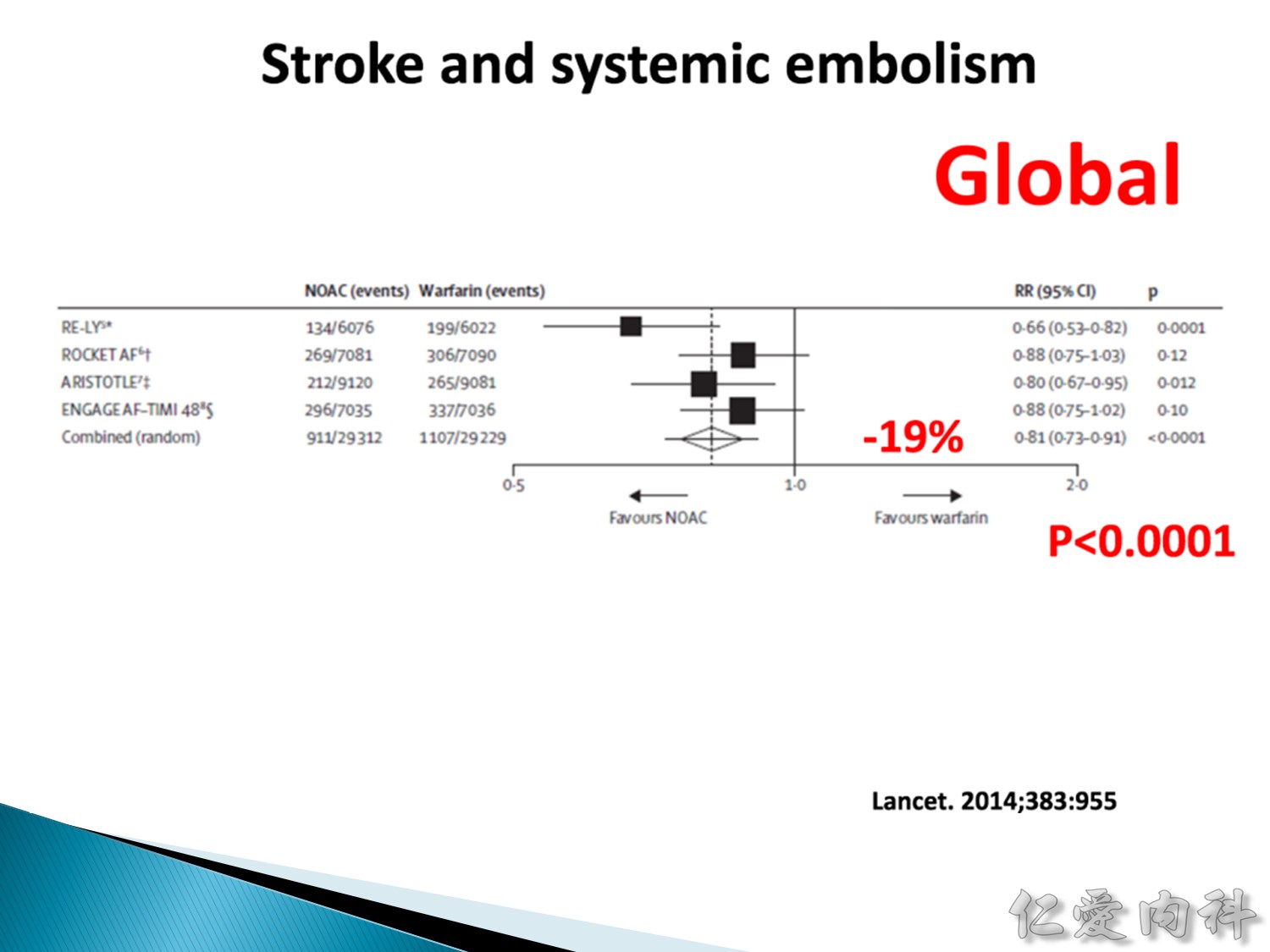
The meta-analysis demonstrated a clear and statistically significant reduction in stroke risk with warfarin compared with placebo.
綜合分析顯示,相較於安慰劑,warfarin 可明顯降低中風風險(具統計顯著性)。
The overall relative risk reduction with warfarin was 64%.
Warfarin 的整體相對風險降幅為 64%。
While the results from the individual trials showed some variability, warfarin more than halved the risk of stroke in five of the six trials.
雖然個別試驗的結果有一些差異存在,但在 6 項試驗中有 5 項顯示 warfarin 可使中風風險降低一半以上。
The risk reductions with warfarin were statistically significant in four of the six trials.
在 6 項試驗中有 4 項顯示 warfarin 的風險降低作用具有統計顯著性。
These results indicate that warfarin can be highly effective in preventing stroke in patients with atrial fibrillation.
這些結果顯示,warfarin 對於心房顫動病患的中風預防具有高度功效。
Ref: Circulation 2006;114:e257-e354
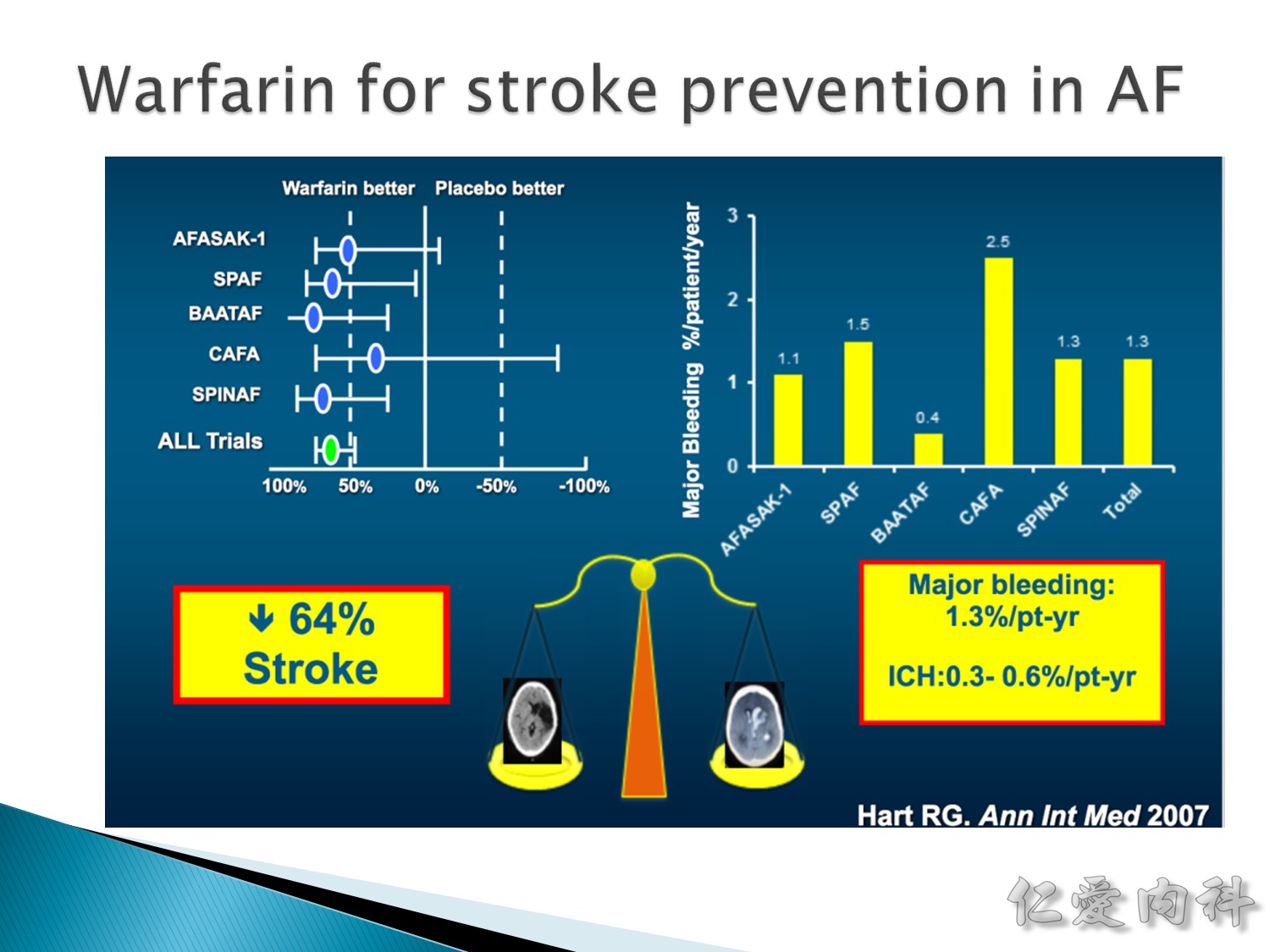
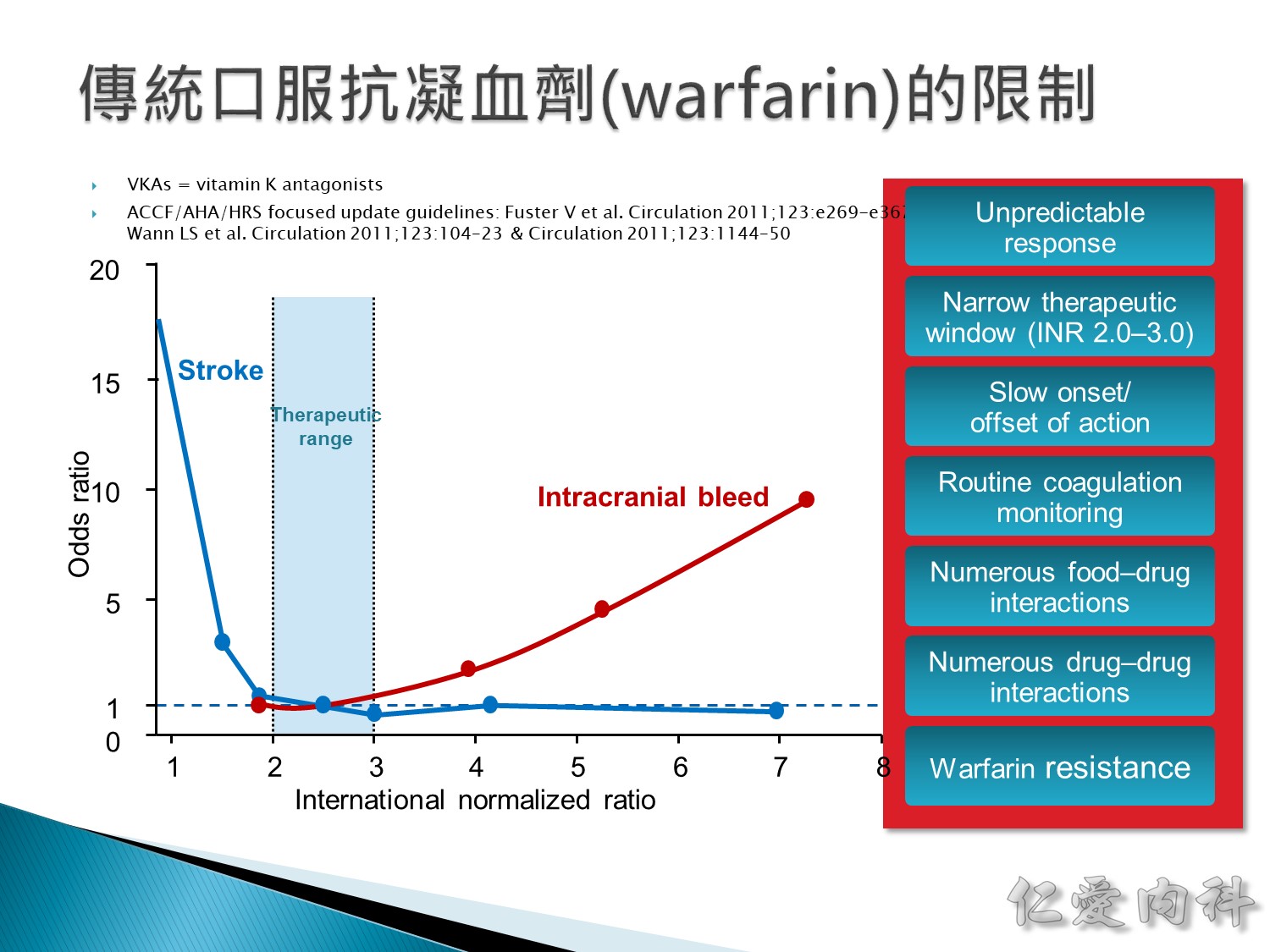
- wafarin 的治療範圍特別的窄
- 一旦要吃這個藥, 1% 的 major bleeding, 0.5% 的 ICH
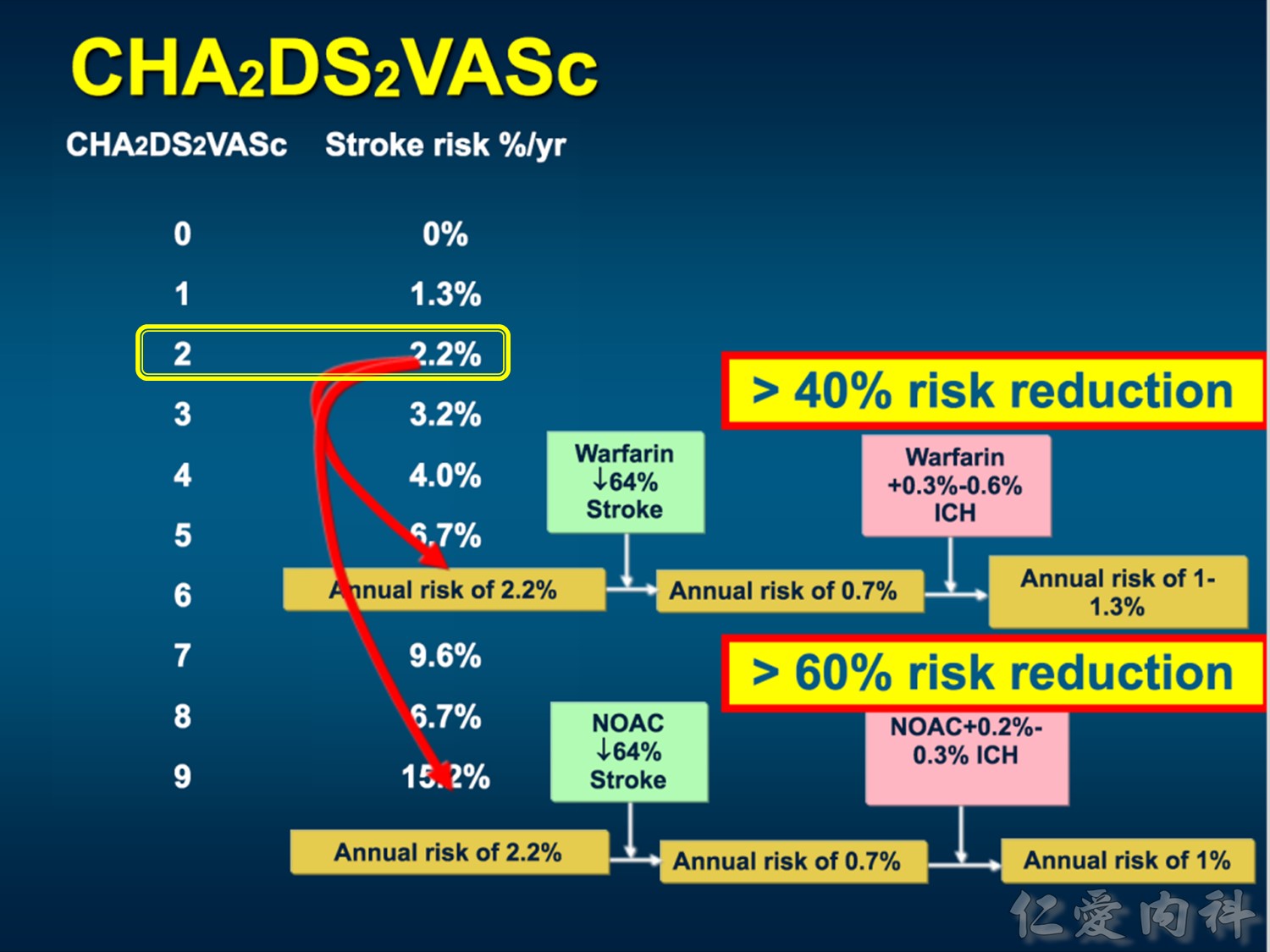
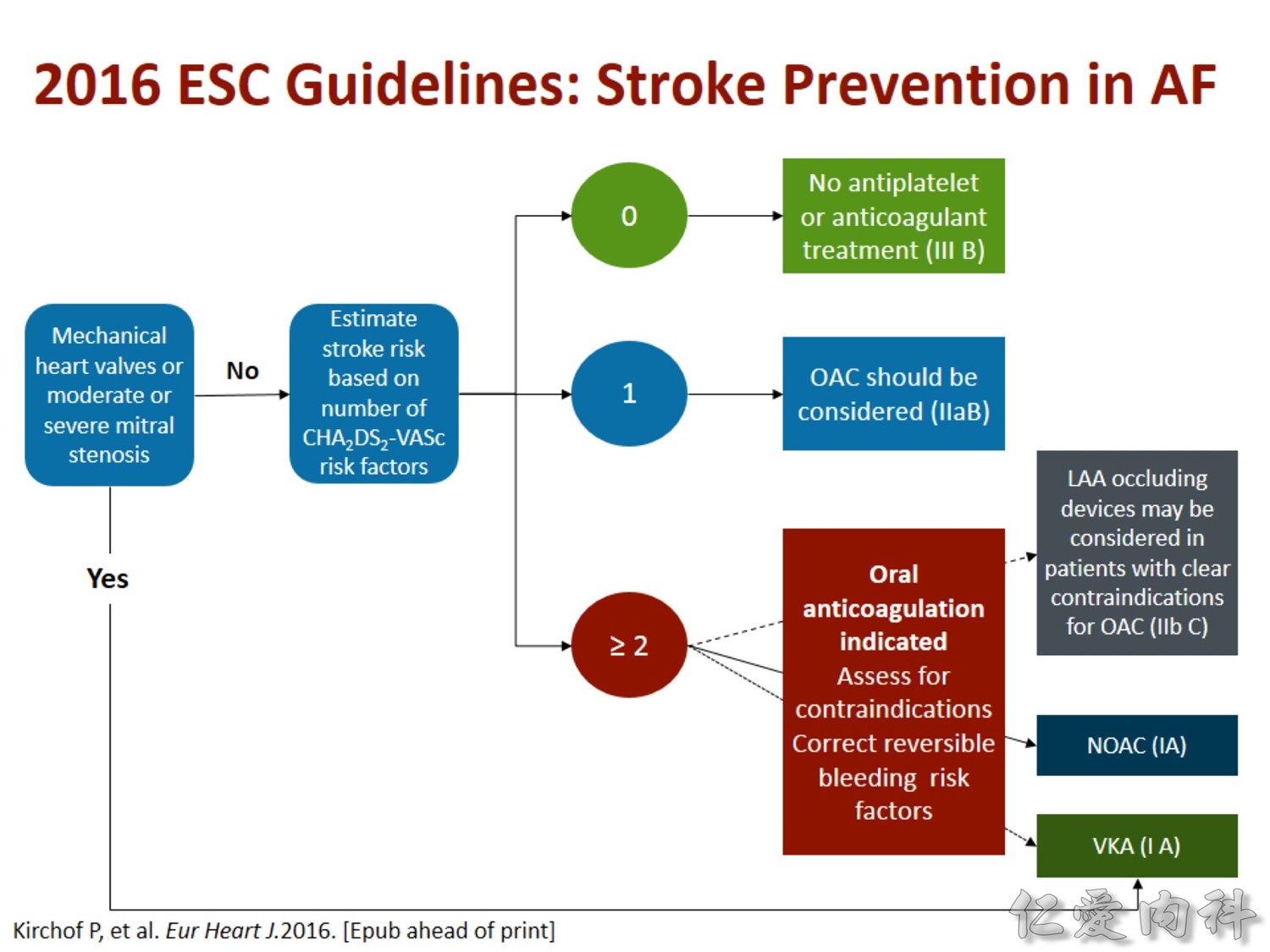
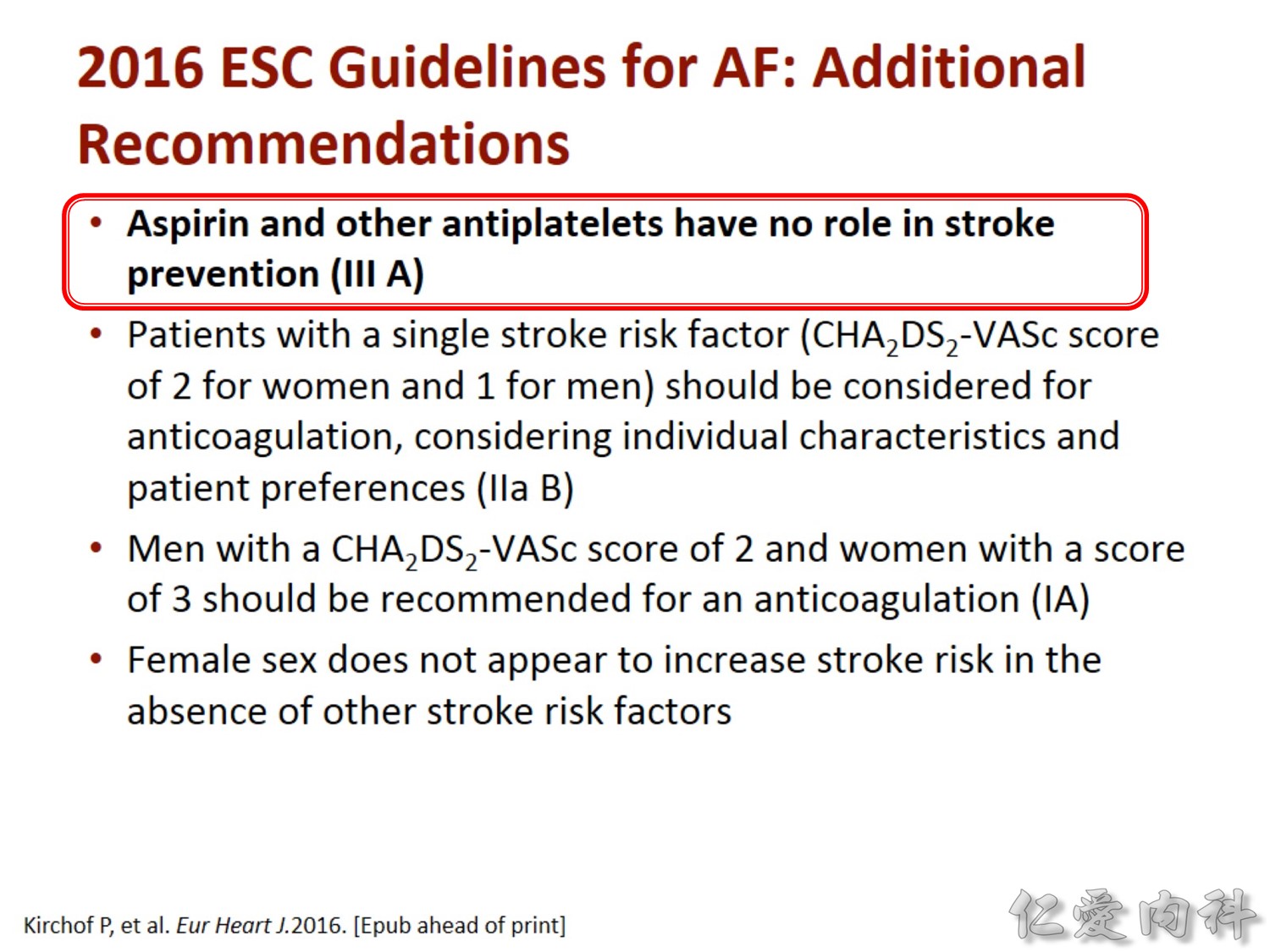
1. 2 分以上:需考慮吃 wafarin 2.2% → 0.7% 中風,,即使加上 ICH,也還是約為 1% → > 40% 降低 Stroke 機率。
2. 2 分以上:吃 NOAC 的話 2.2% → 0.7% 中風→ > 60% 降低 Stroke 機率。
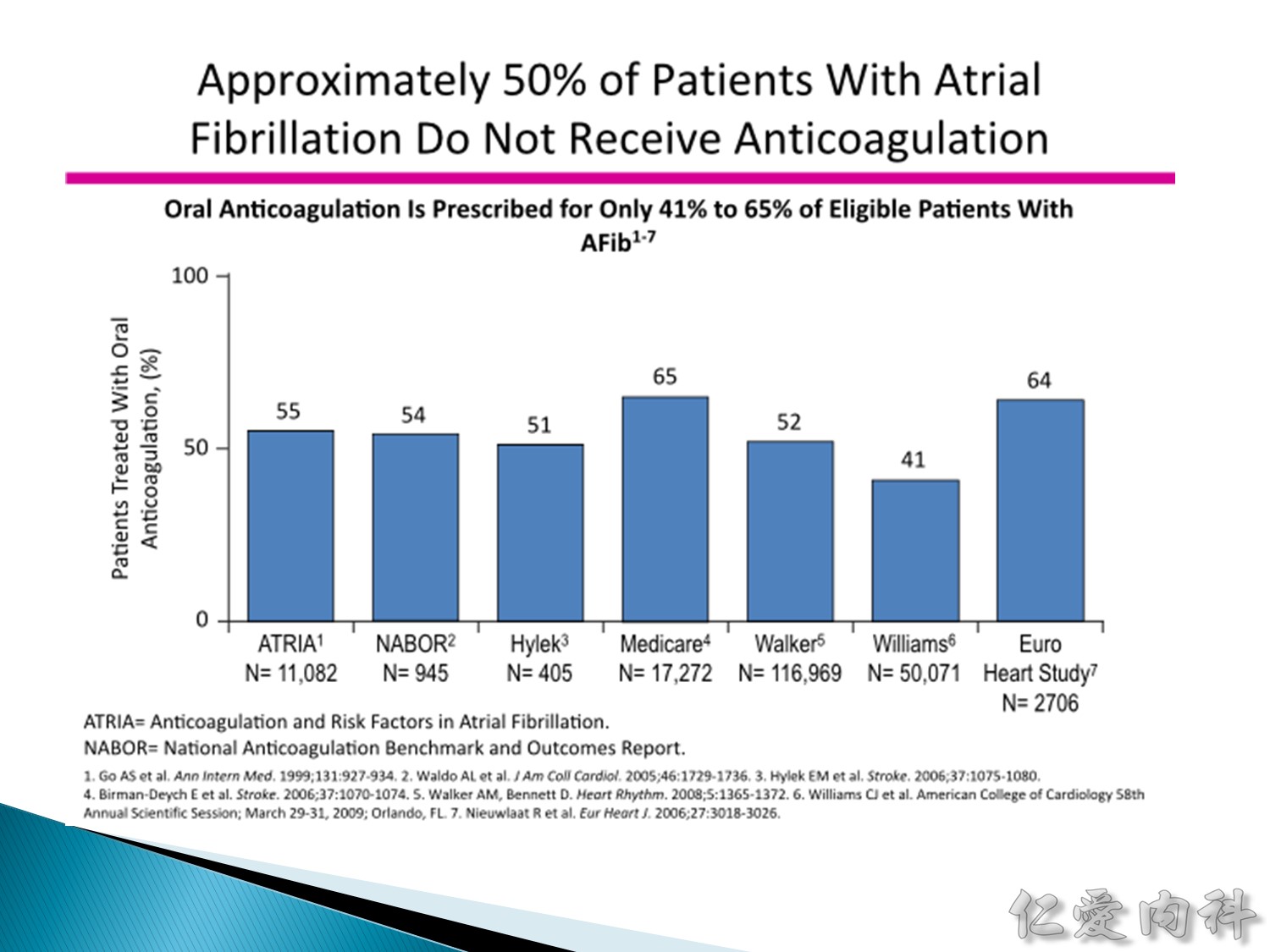
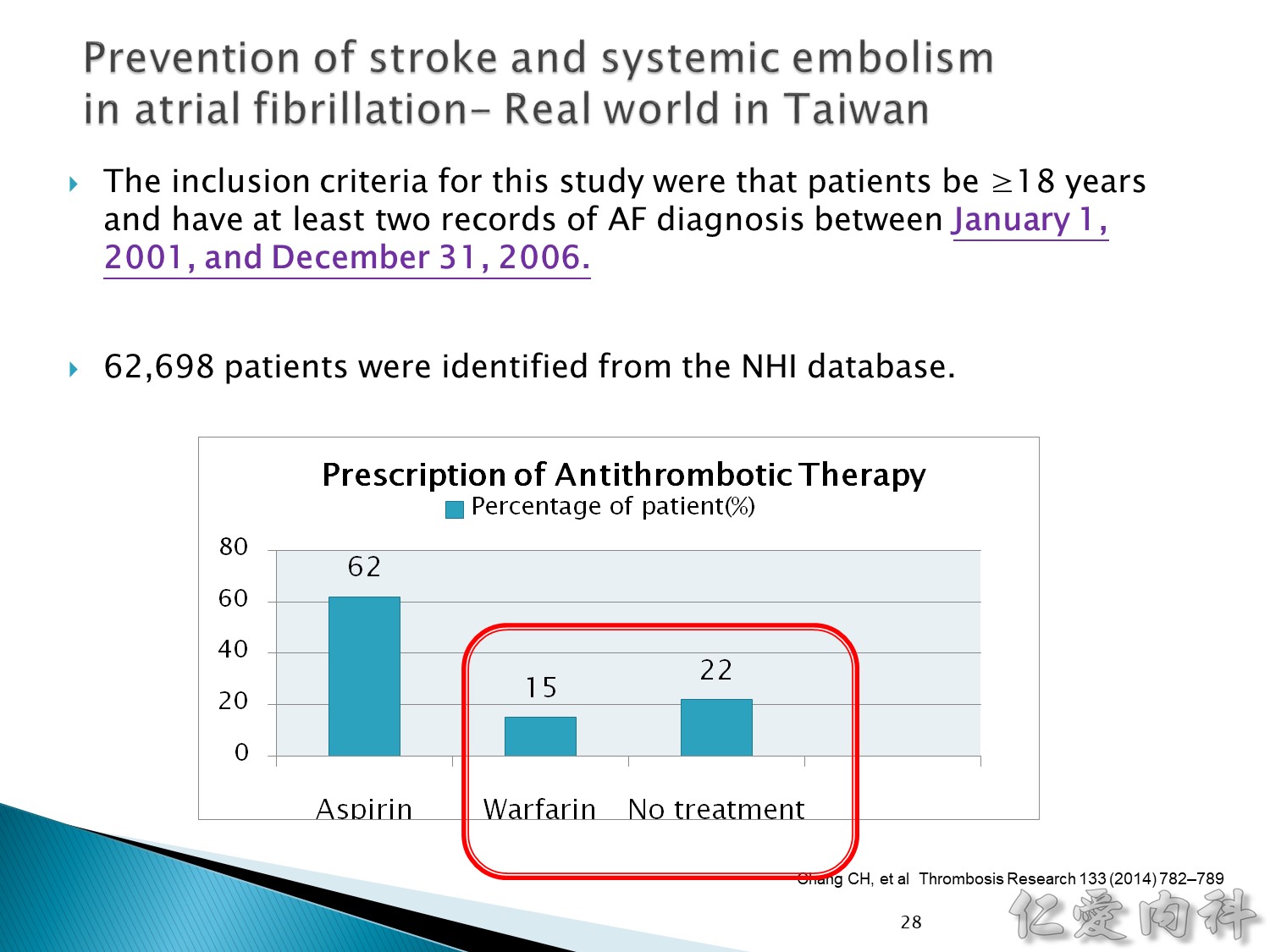
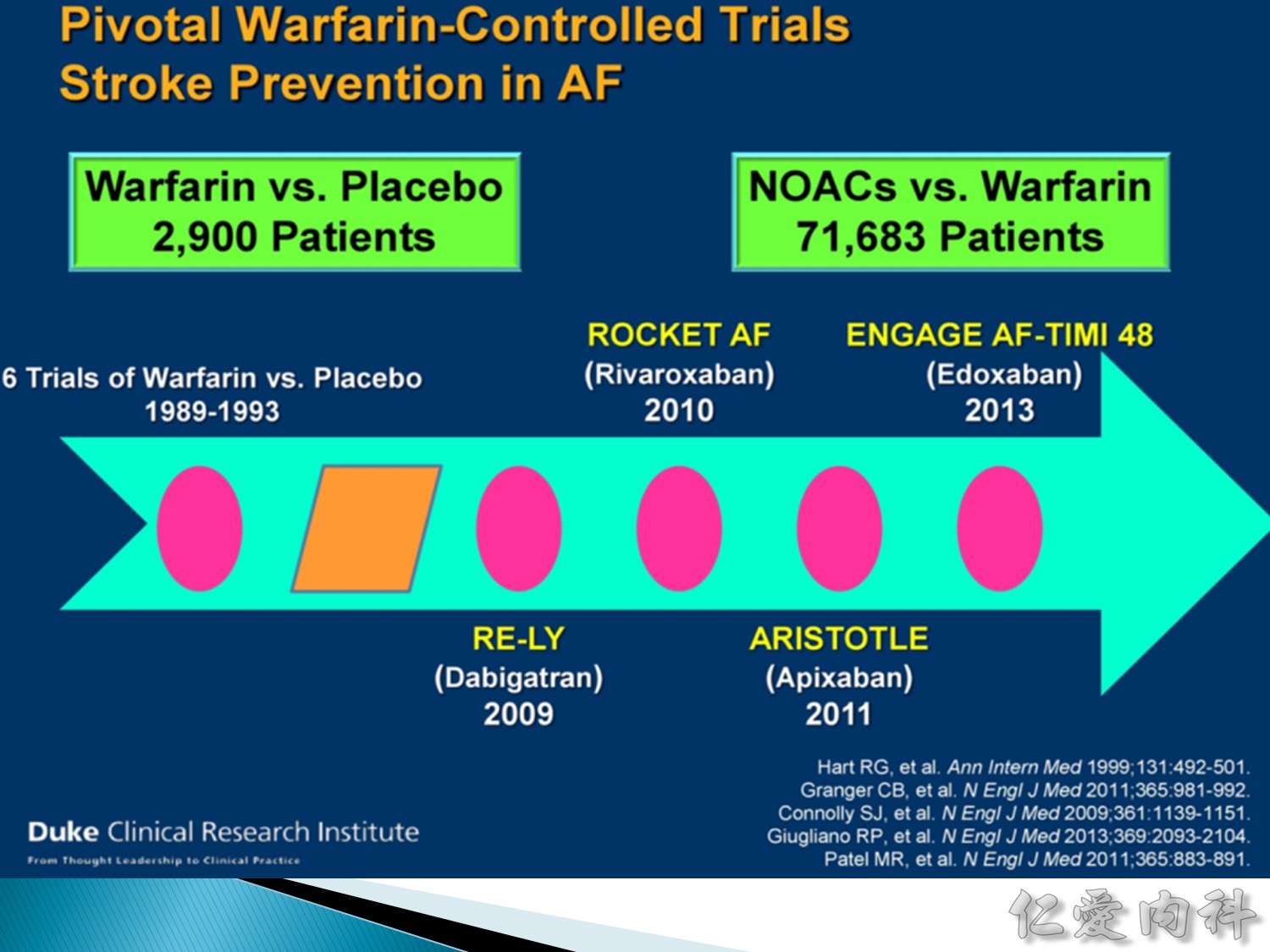
在 clinical trial 裡面,有 Afib 的病人還有將近一半的比例沒有接受抗凝血劑的藥物。
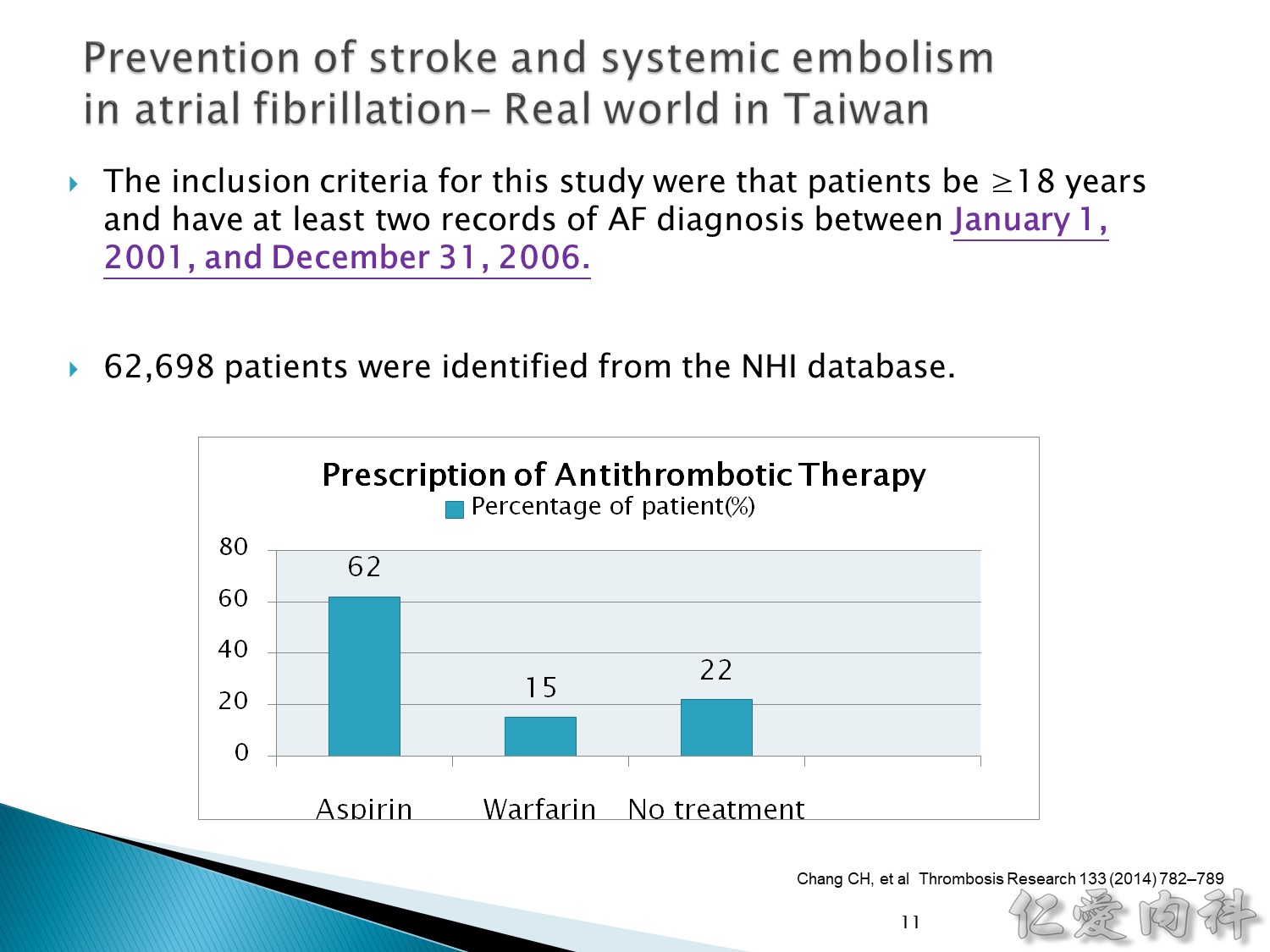
在 2014 年的台灣統計,真正使用 wafarin 的只有 15%,真正有得到良好治療的比例很低。
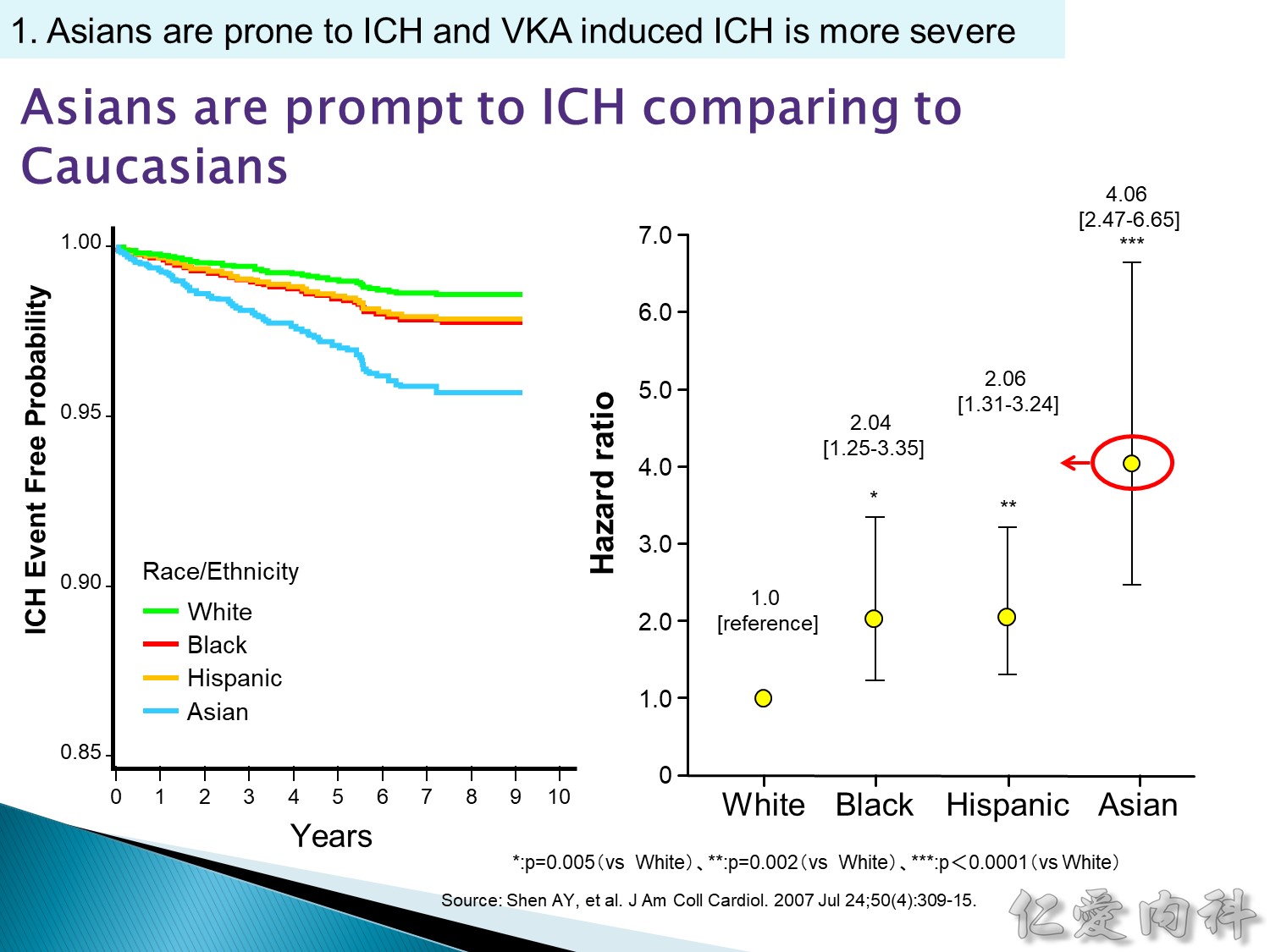
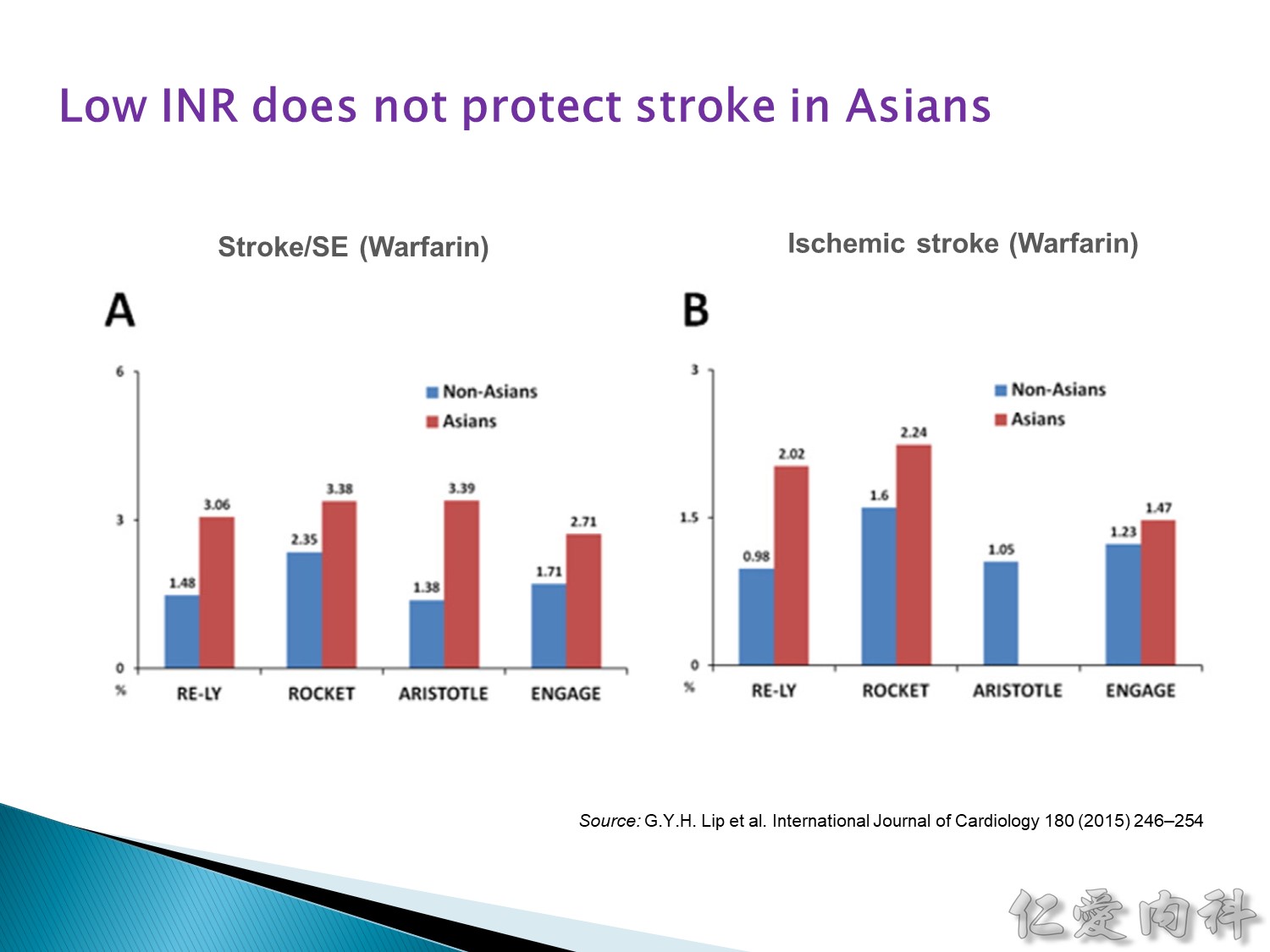
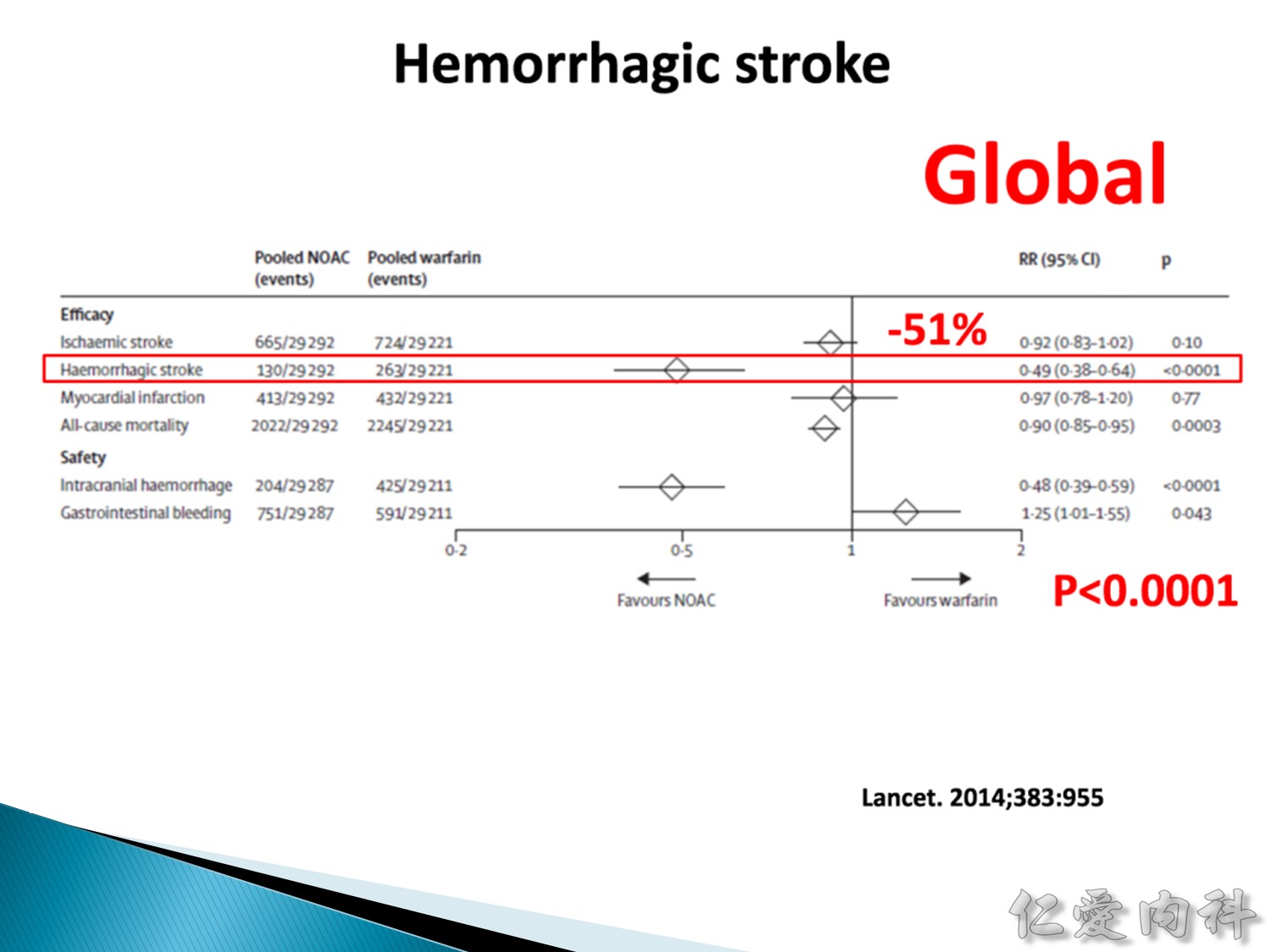
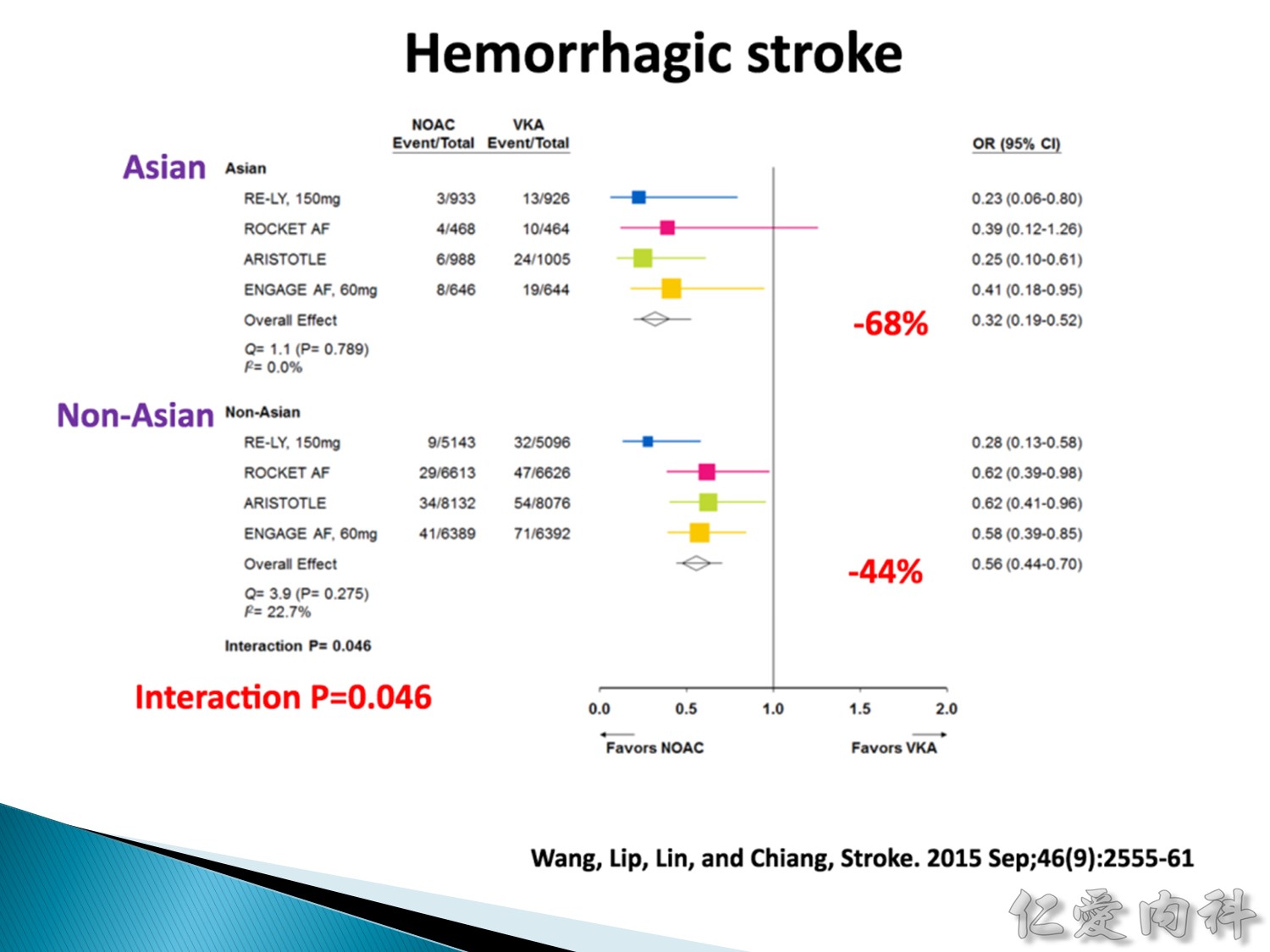
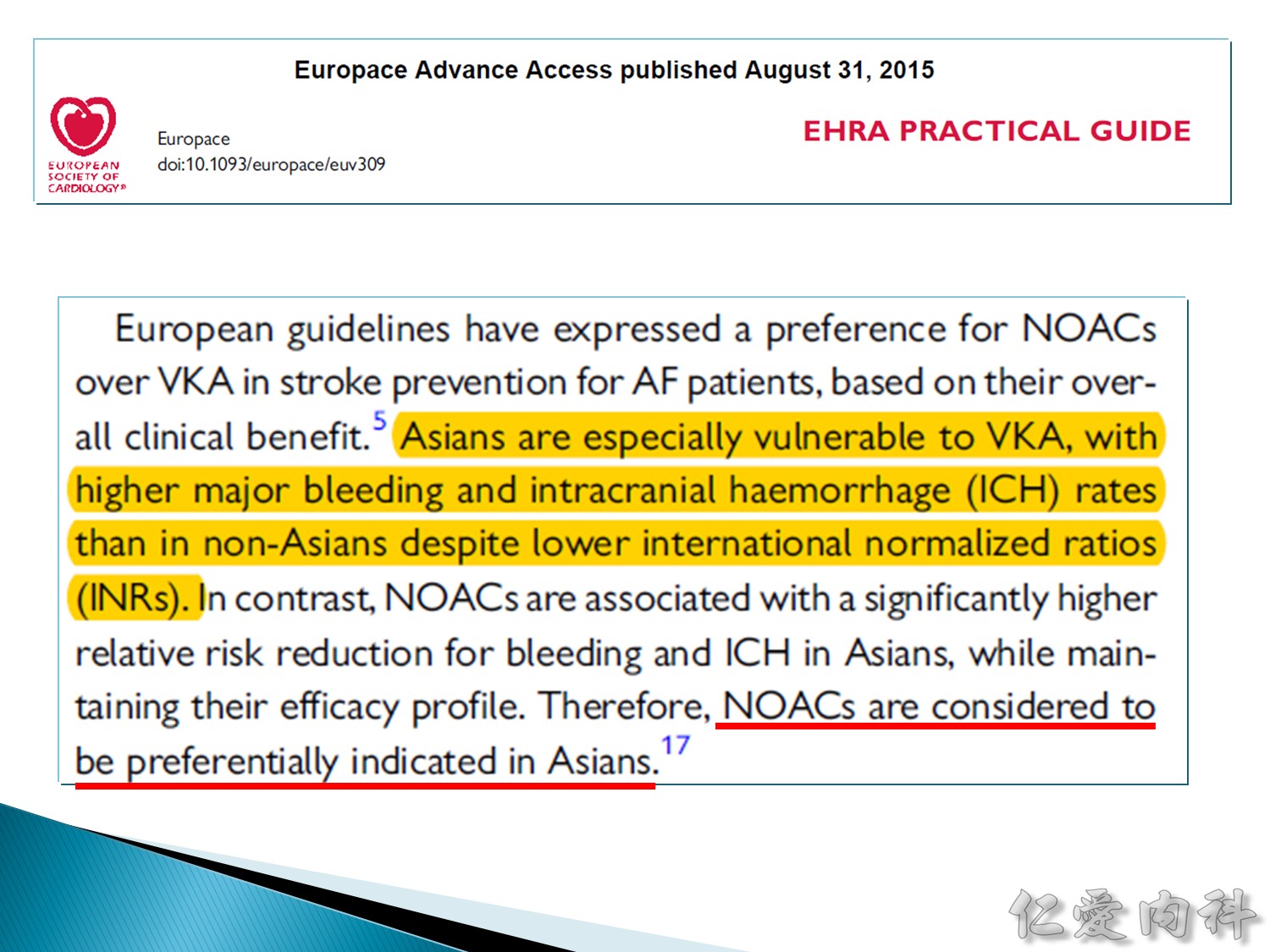
亞洲人相對於白種人 ICH 的機會是白種人的 4 倍。
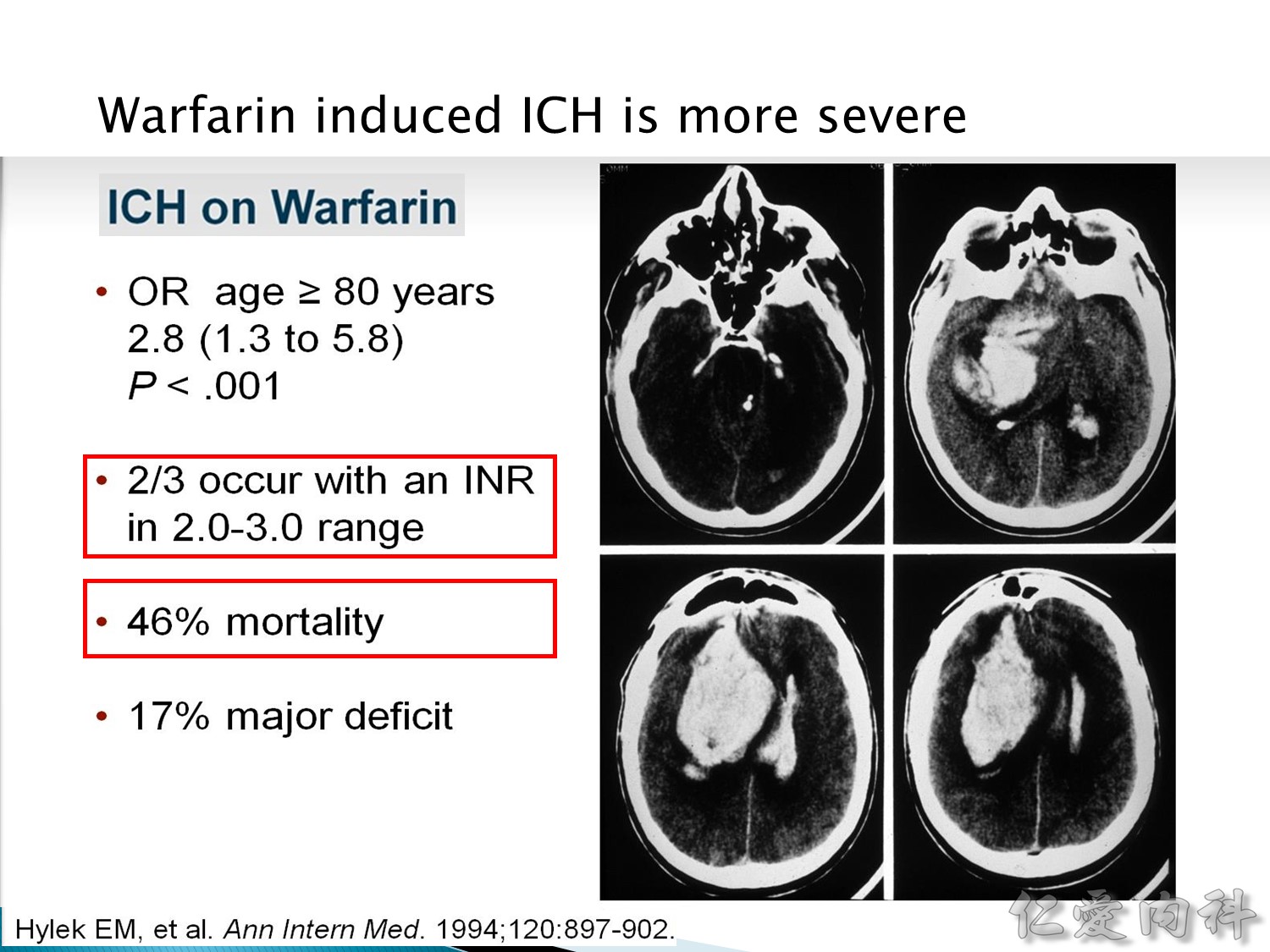
吃 wafarin 的話,死亡率約 46%,沒掛掉也 major deficit,很多吃 warfarin 的病人ICH 的病人 INR 都在正常範圍內 (2-3)。
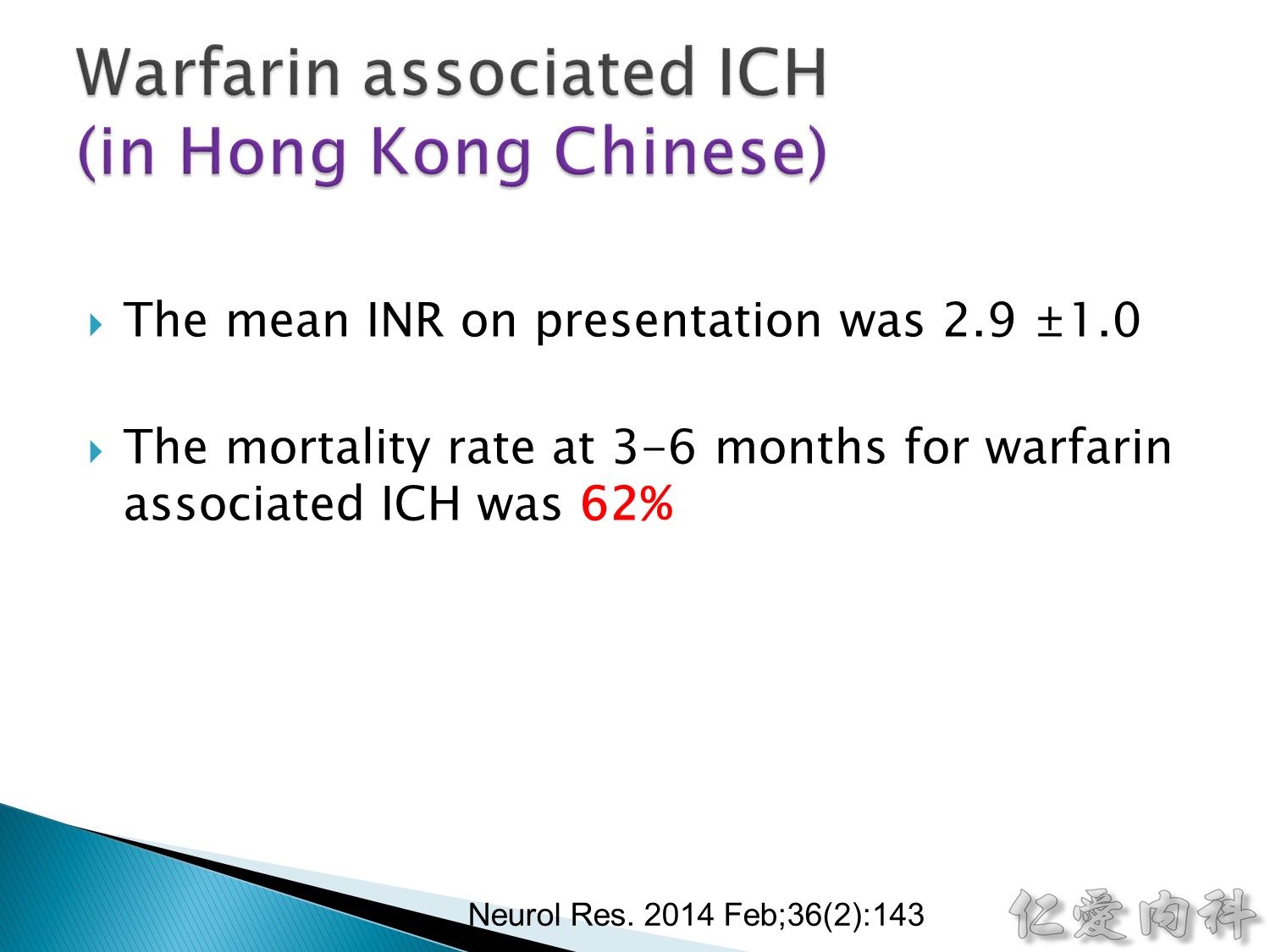
香港的統計,死亡率是 62%,mean INR 也是 2.9
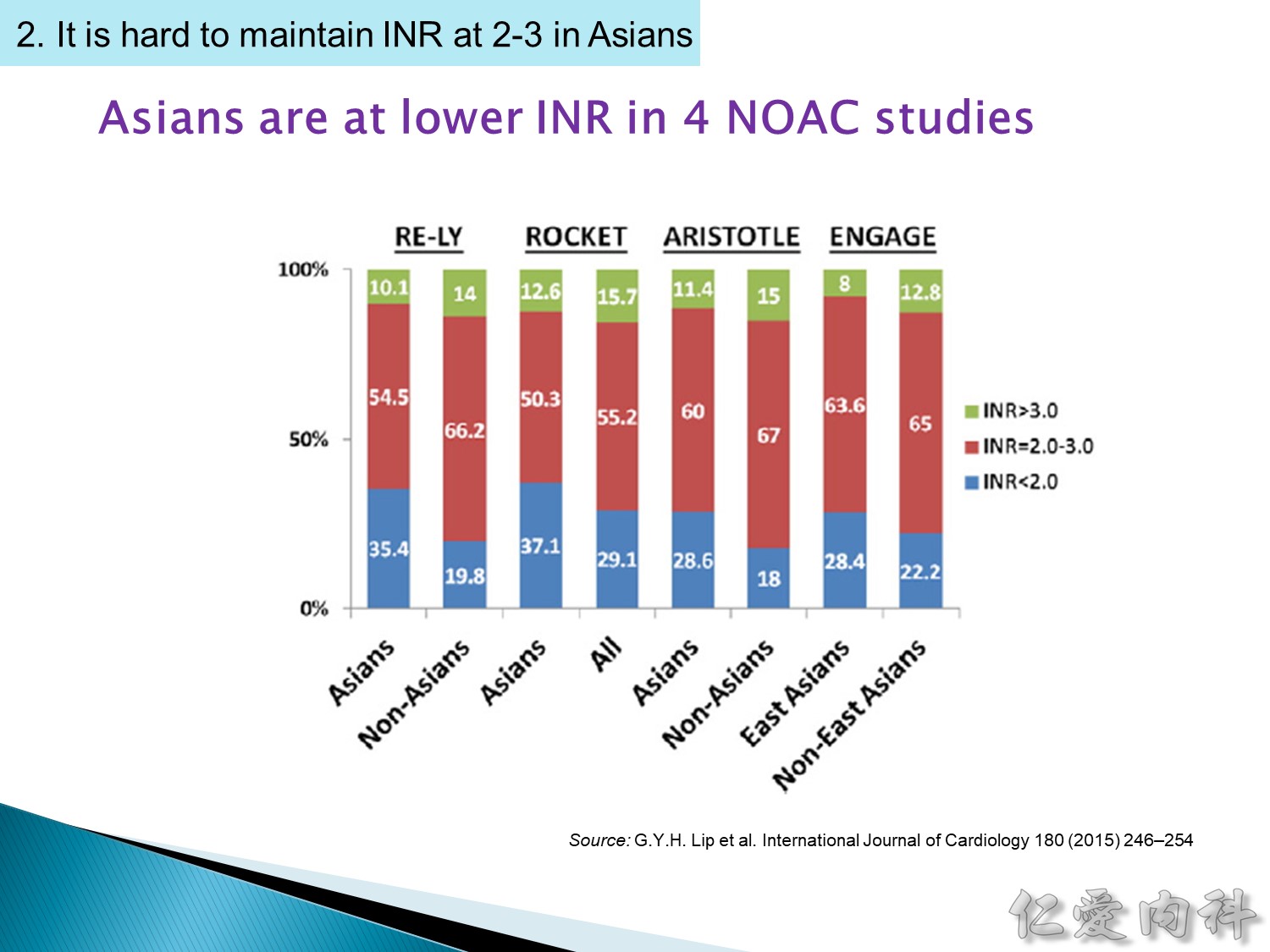
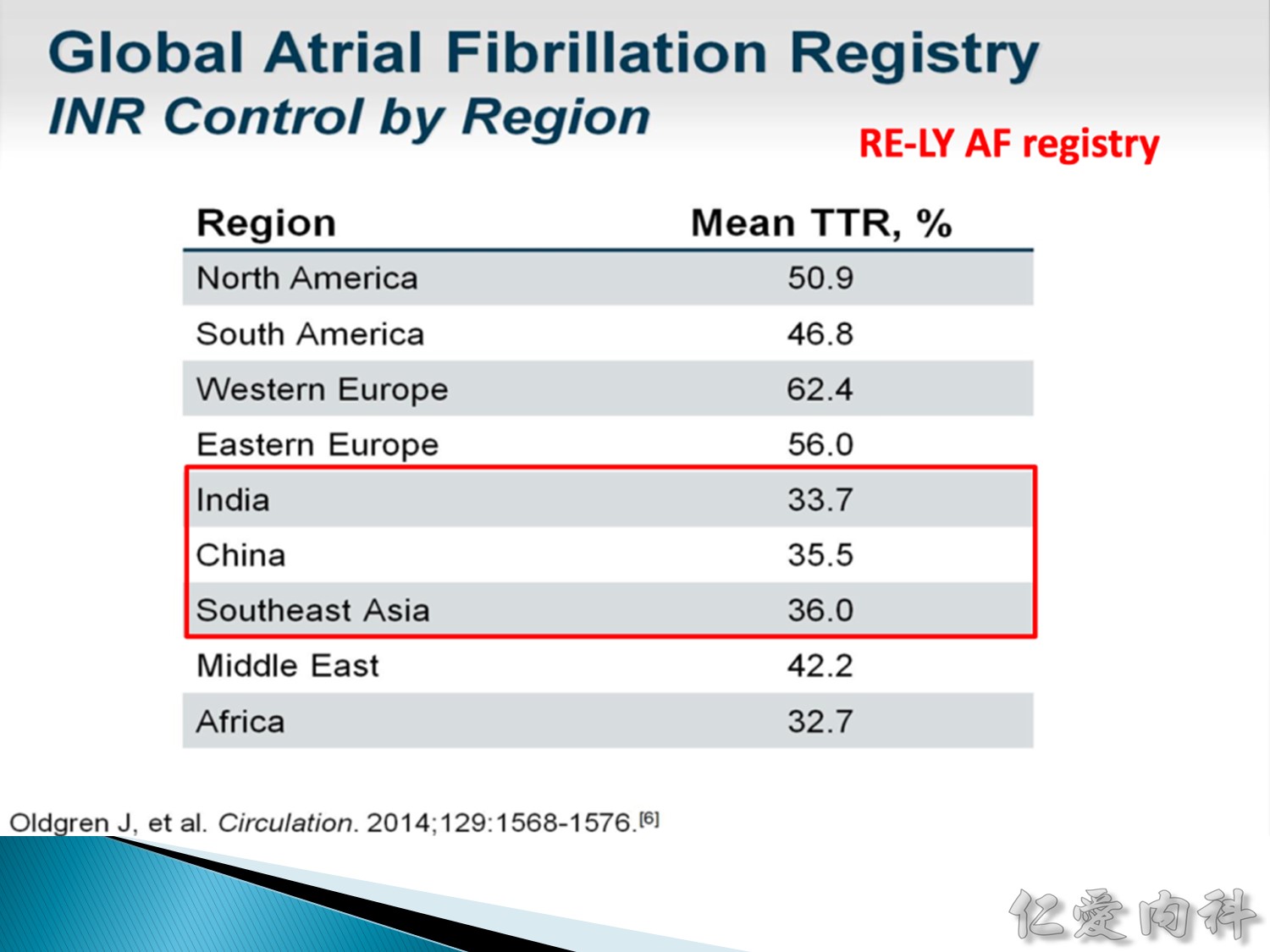
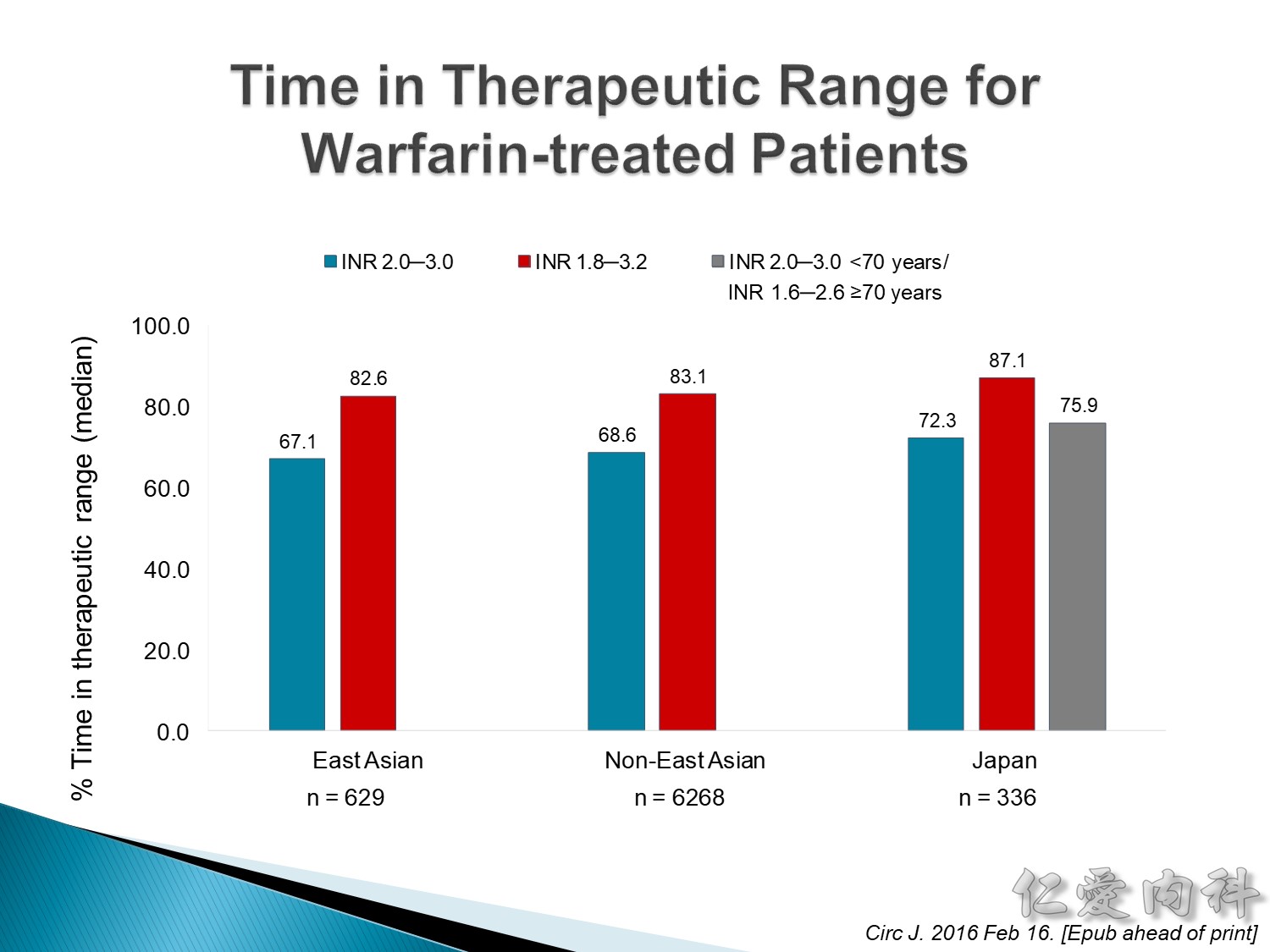
維持 INR 在正常比例內的很困難,guideline 要求 warfarin 的治療要求 TTR (time in therapeutic range) 需要在 65% 以上,抽 10 次血要有 6.5 次需要 INR 在 2-3 之間。
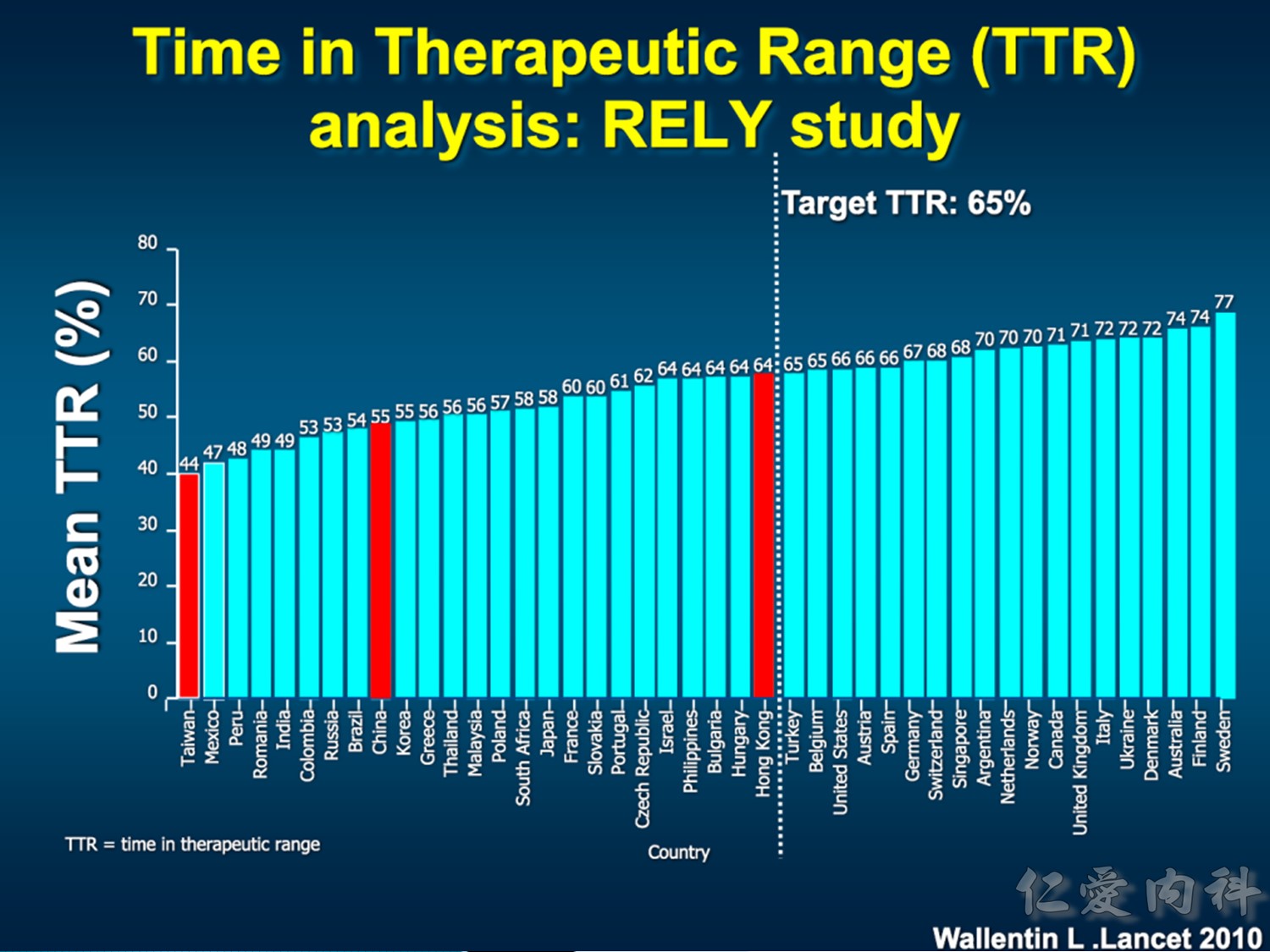
即使是 clincal trial,台灣的 TTR 都還是不足的。
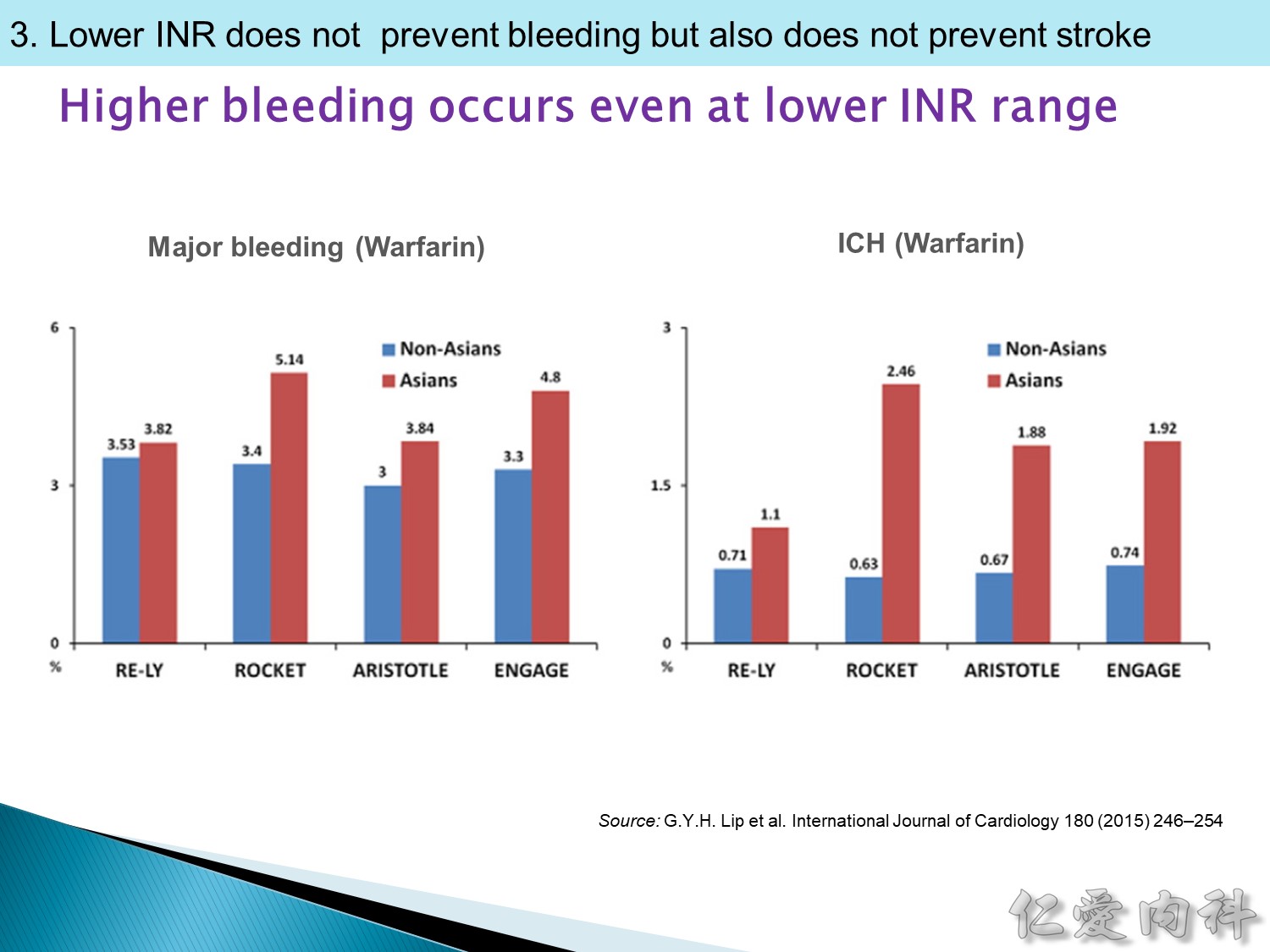
亞洲的醫生會把 INR 控制更低一點,但 ICH 還是比非亞洲人來的高,結果 ischemia stroke 也沒有降低。
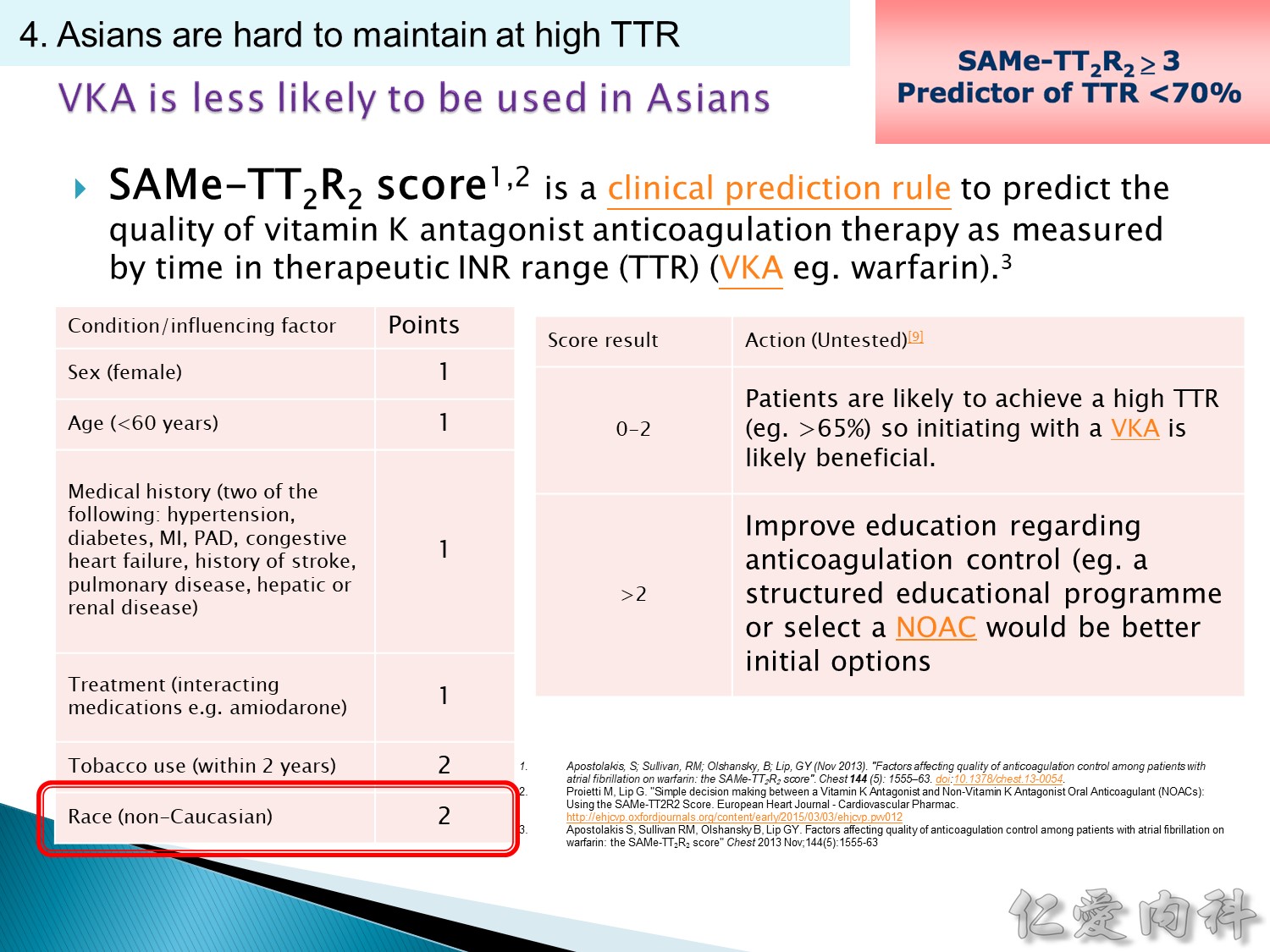
預測一個人使用 warfarin 後,是否能夠達到治療藥物,亞洲人每個都 2 分,SAMe-TT2R2 score > 3,TTR 要 > 70%基本不太可能,只要是亞洲女性就不太適合使用 warfarin。
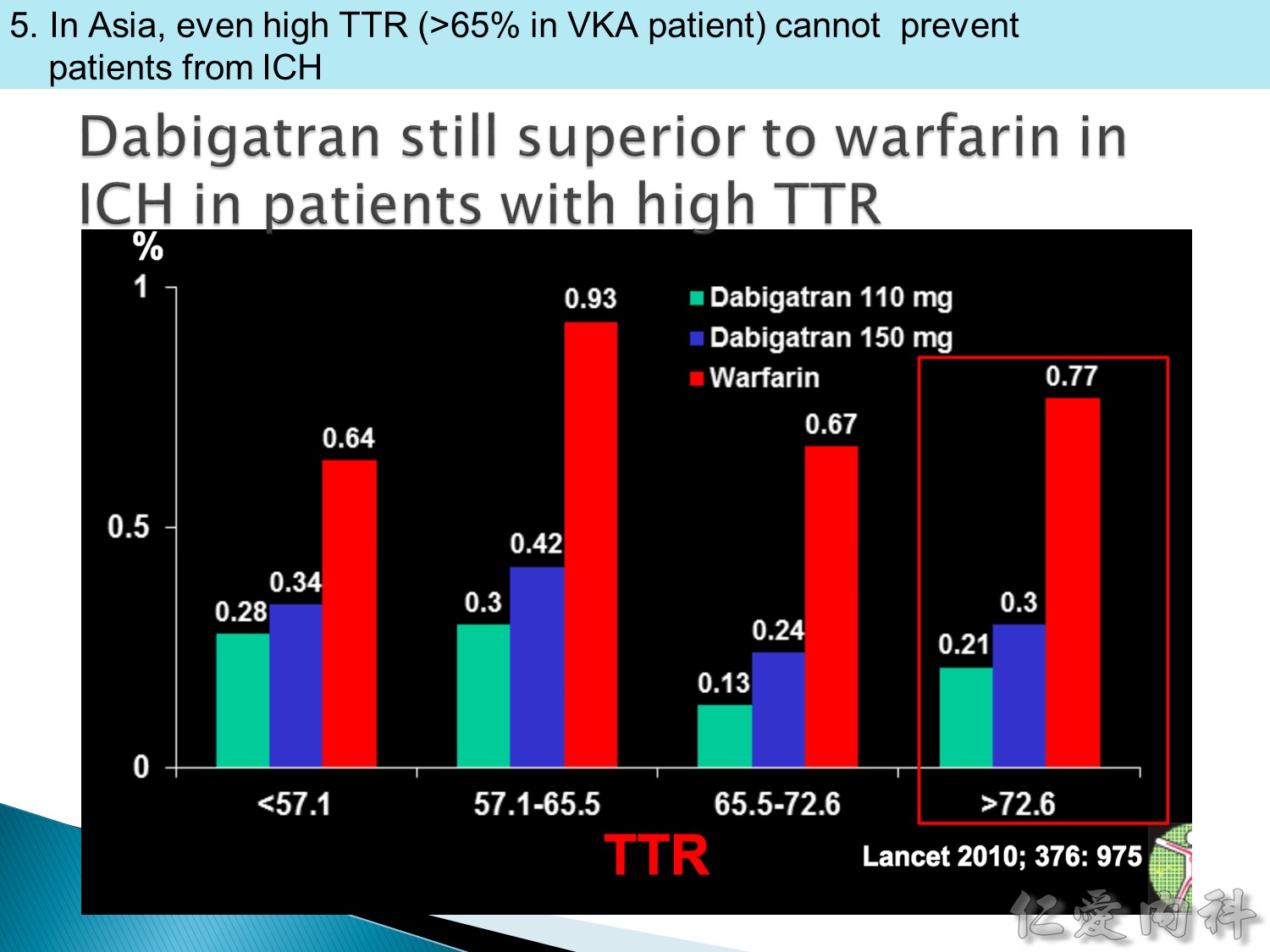
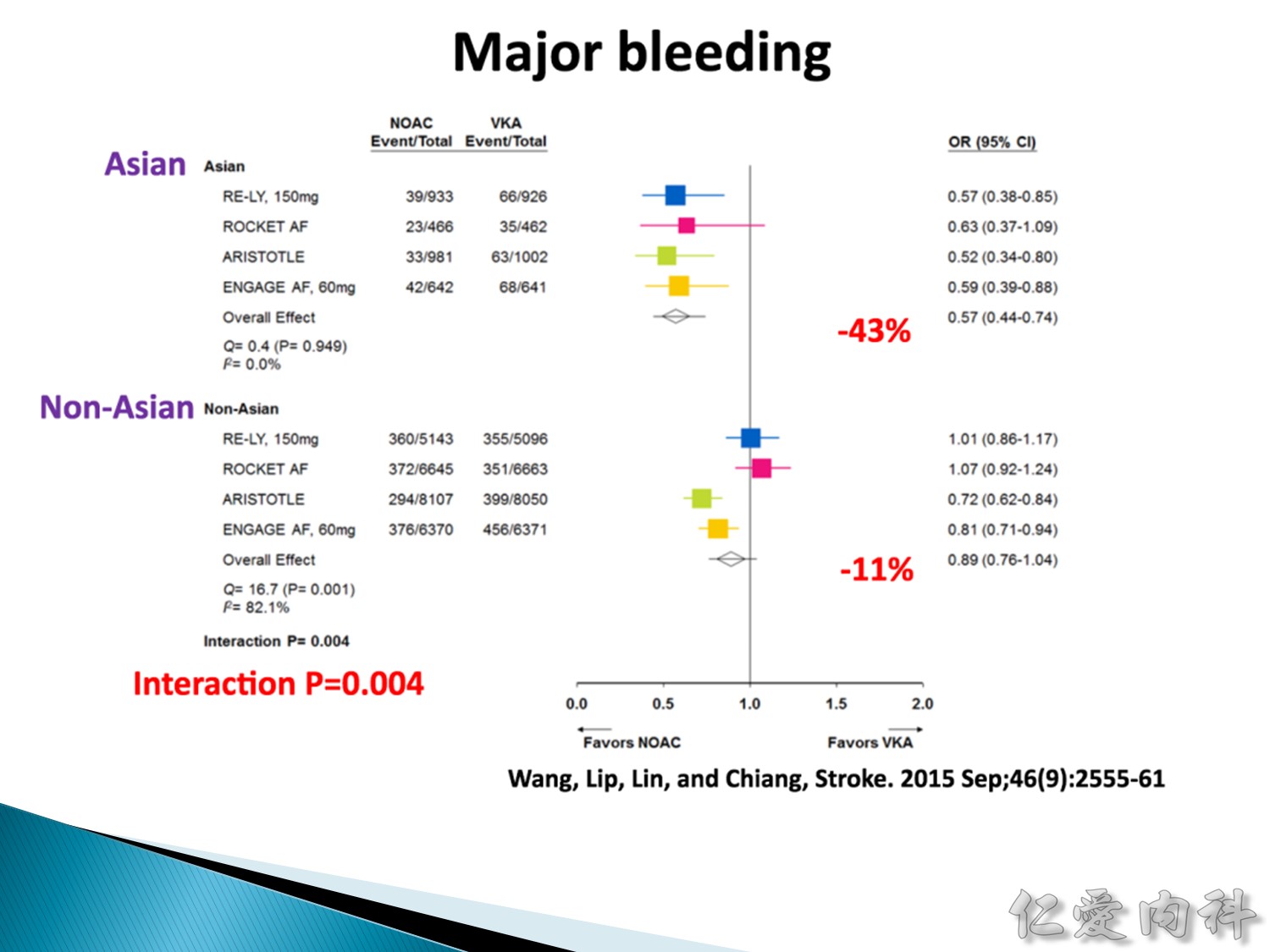
1. 在亞洲人身上,即使 warfarin 的 TTR 控制得很好,但出血機率還是比 NOAC 來的高。
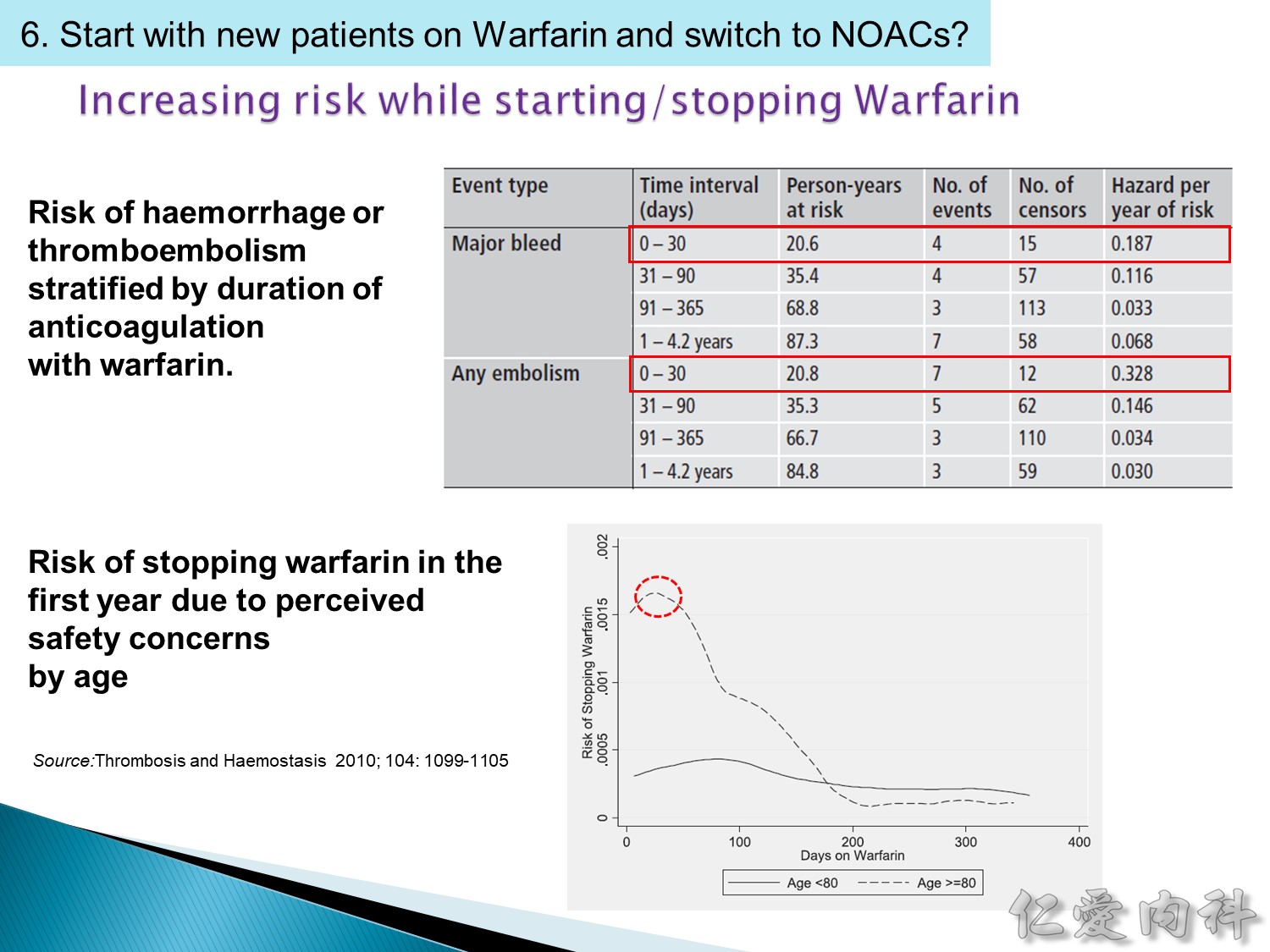
2. warfarin 剛開始時為什麼跟 heparin or LMWH (low molecular weight heparin) 最好要有overlap,因為剛開始用時,反而會增加 thrombotic rate (warfarin loading 會減少 protein C and S 而造成 hypercoagulation 所以需要 overlapping)。
During commencement of oral VKA therapy a there is a transient hypercoagulable state when the patients are at high risk of further thromboembolic disease. This is due to the difference in plasma halflives between the vitamin K-dependent pro-coagulation factors II and X, and the vitamin K-dependent anticoagulant proteins C and S. The antithrombotic effect of warfarin, caused primarily by a reduction in the activity of factor II, is delayed for as long as 72 to 96 hours. Protein C has a half-life of 6 hours and decreases at the same rate as factor VII in the first three days of therapy. Higher doses of warfarin initially may rapidly deplete protein C prior to adequate suppression of factors II and X. Similarly protein S activity is markedly reduced after initiation of warfarin therapy, reaching a nadir at 46 hours. During this phase of treatment, low levels of proteins C and S in association with inadequate suppression of factors II and X incurs a high risk of thrombosis. There is therefore a prothrombotic phase early on after initiation of warfarin therapy. It is therefore important to overlap heparin and warfarin treatment for at least 48 hours after therapeutic INR values have been achieved to cover the period of hypercoagulability until a balance in favour of antithrombotic effects of warfarin is achieved. (Ref: J Clin Case Rep 3:e121.)
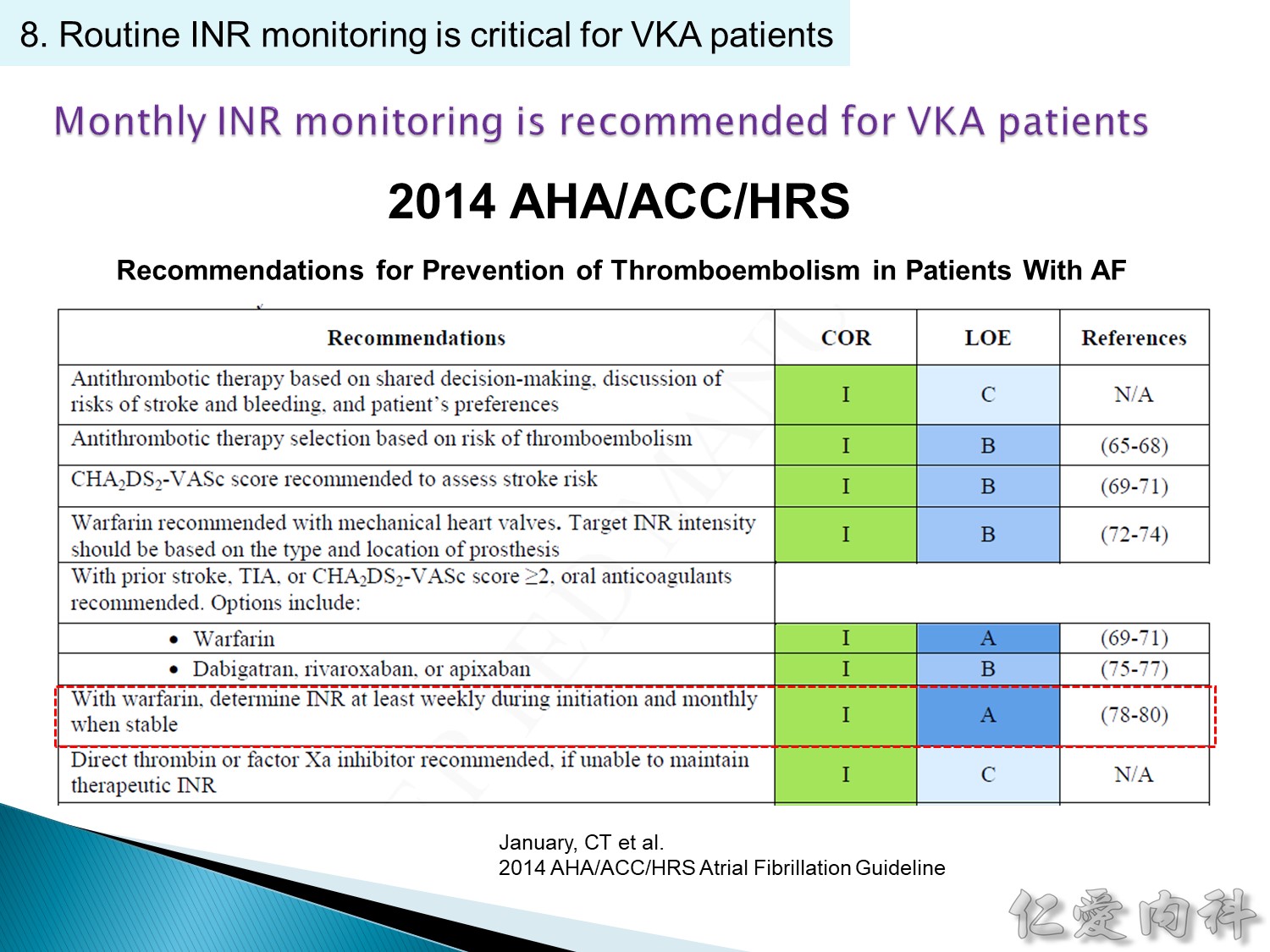 剛開始用 weekly 抽血,穩定後 monthly 抽血。
剛開始用 weekly 抽血,穩定後 monthly 抽血。
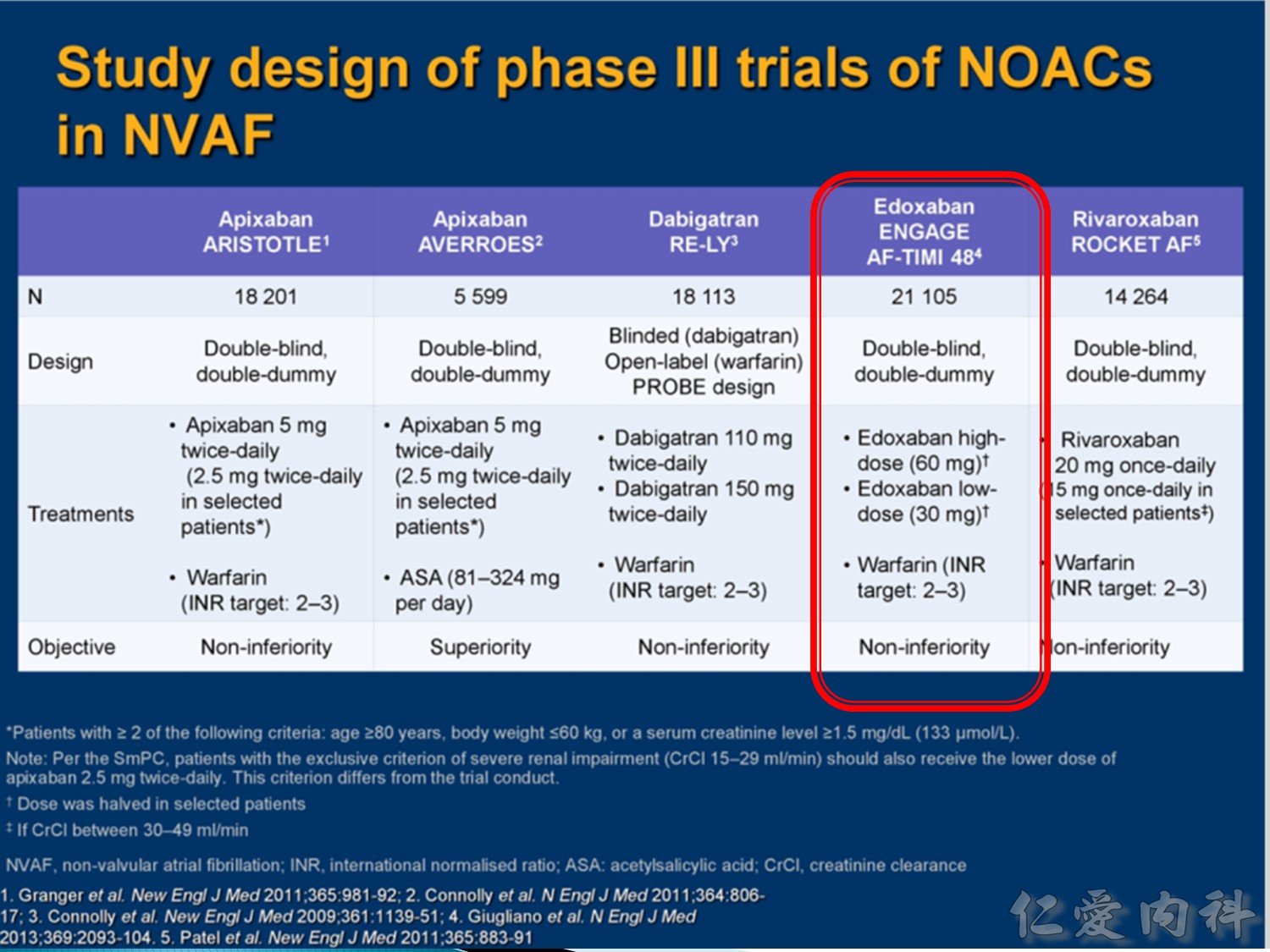
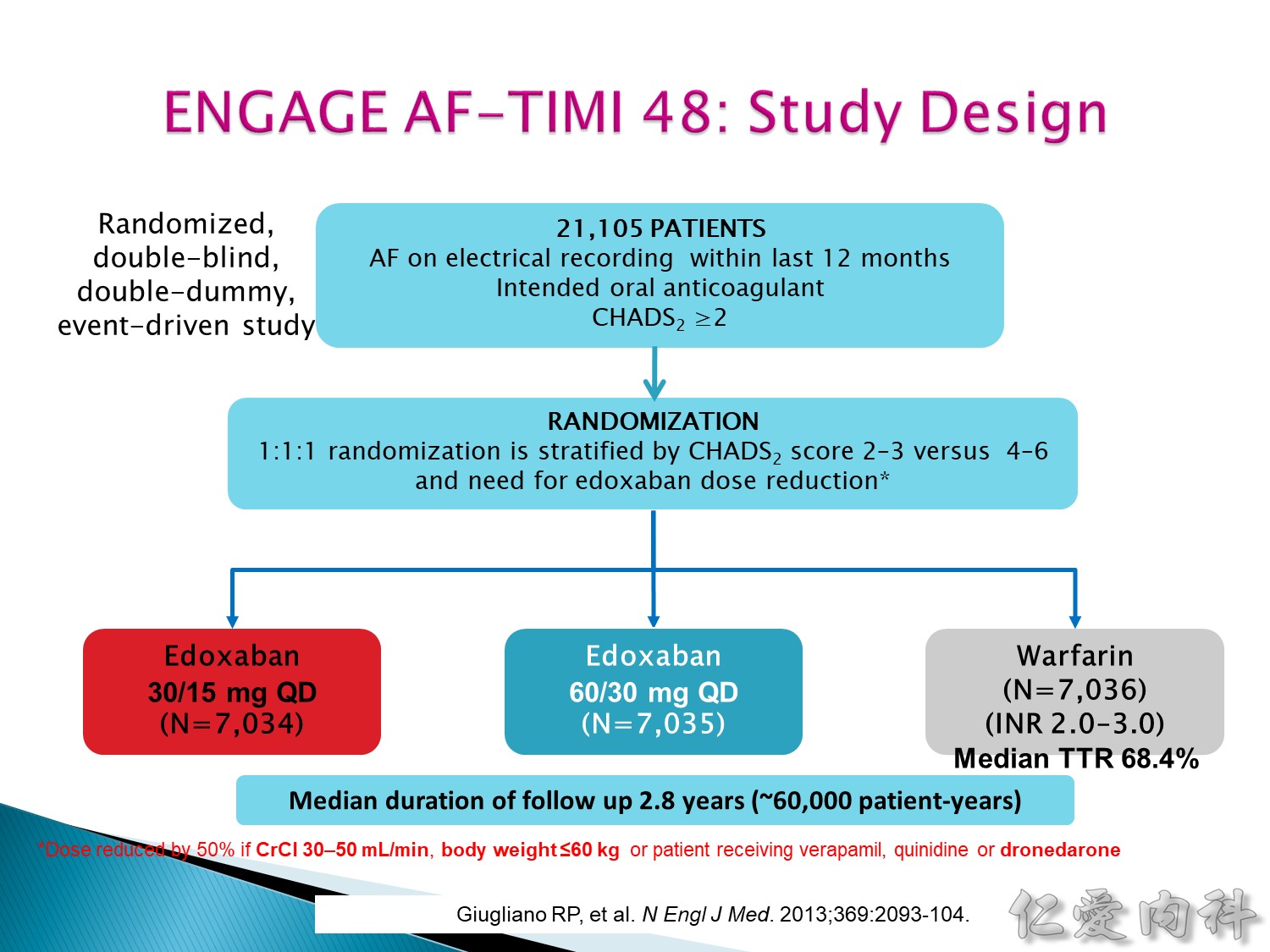
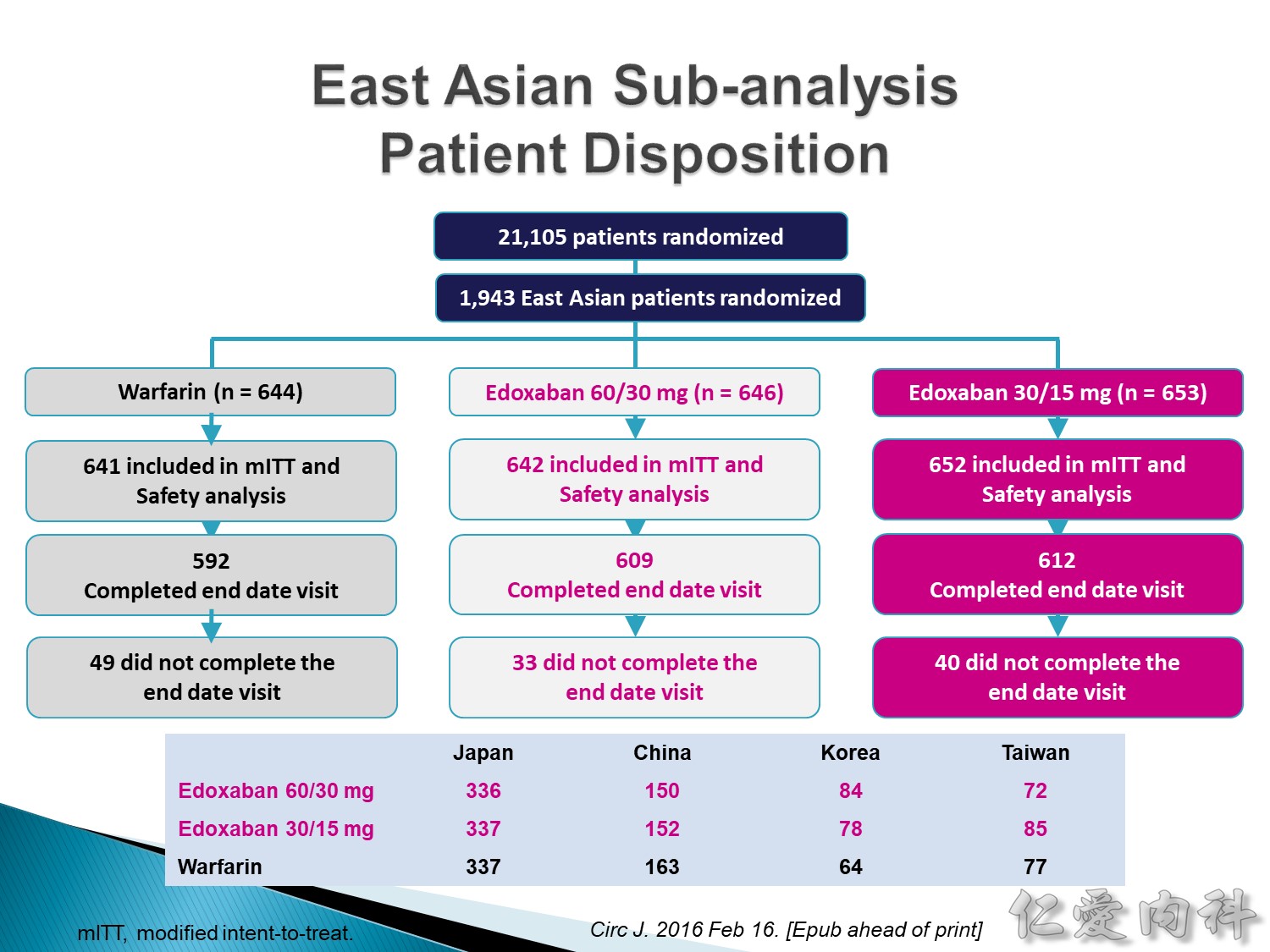
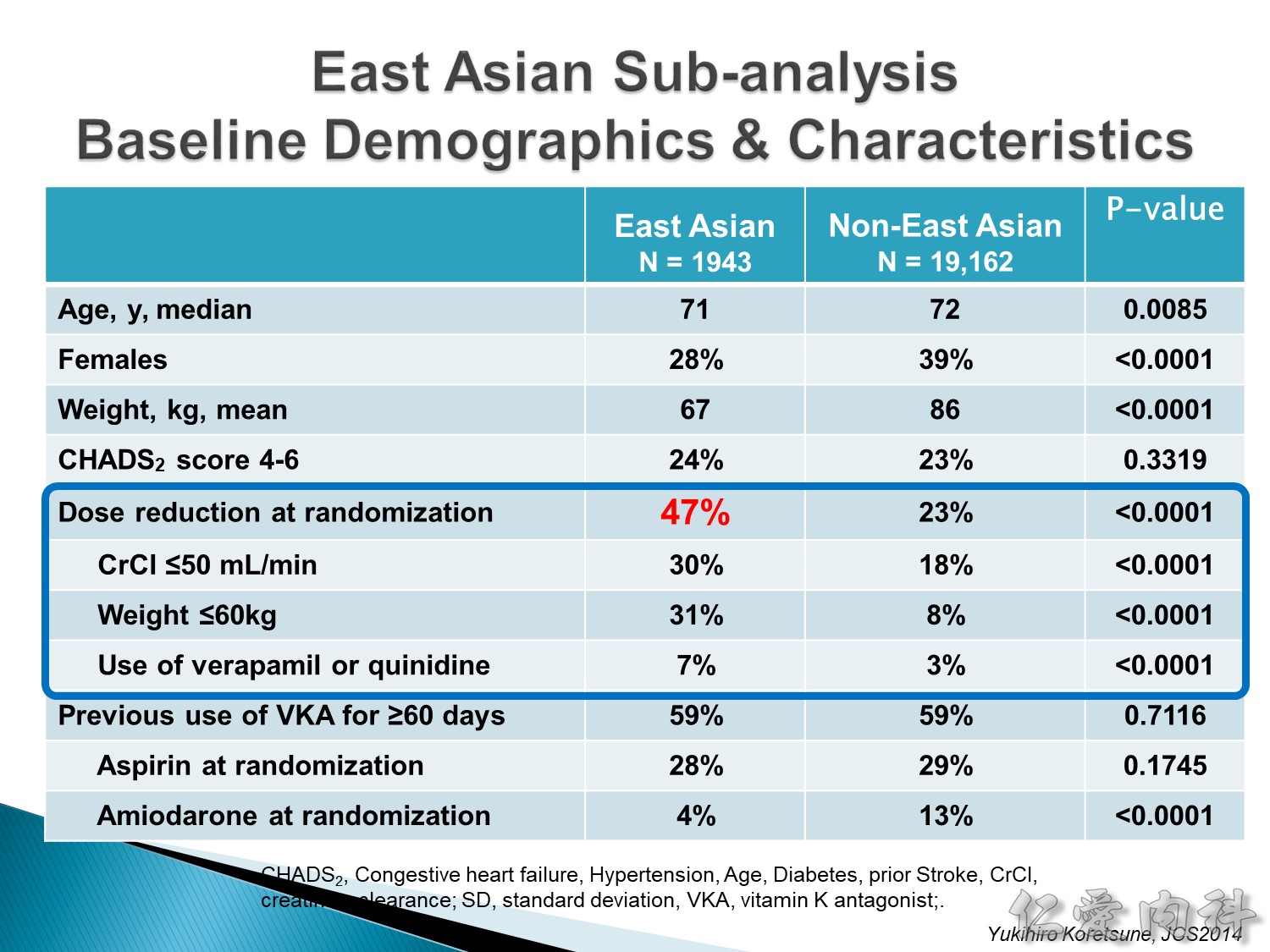
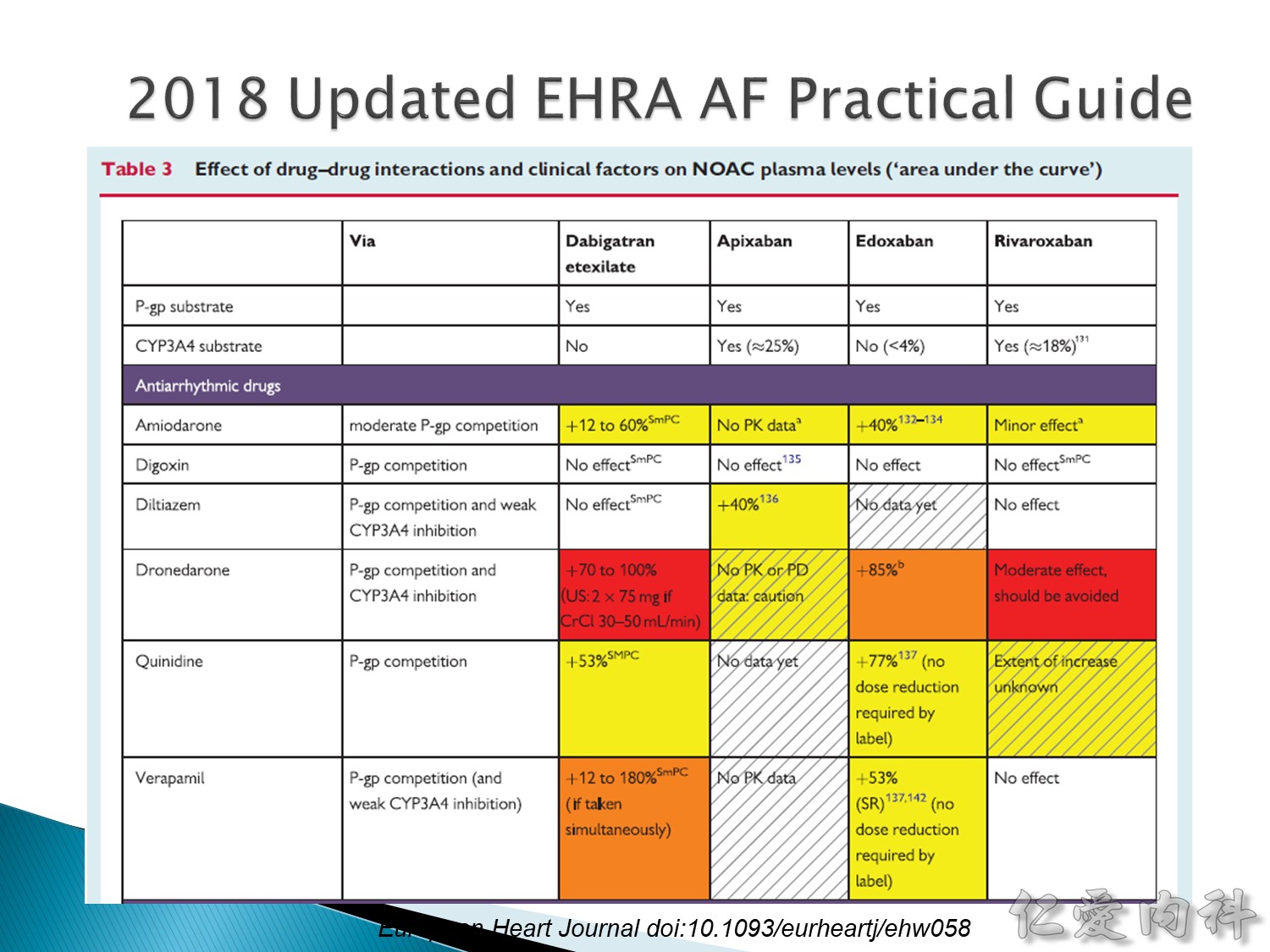
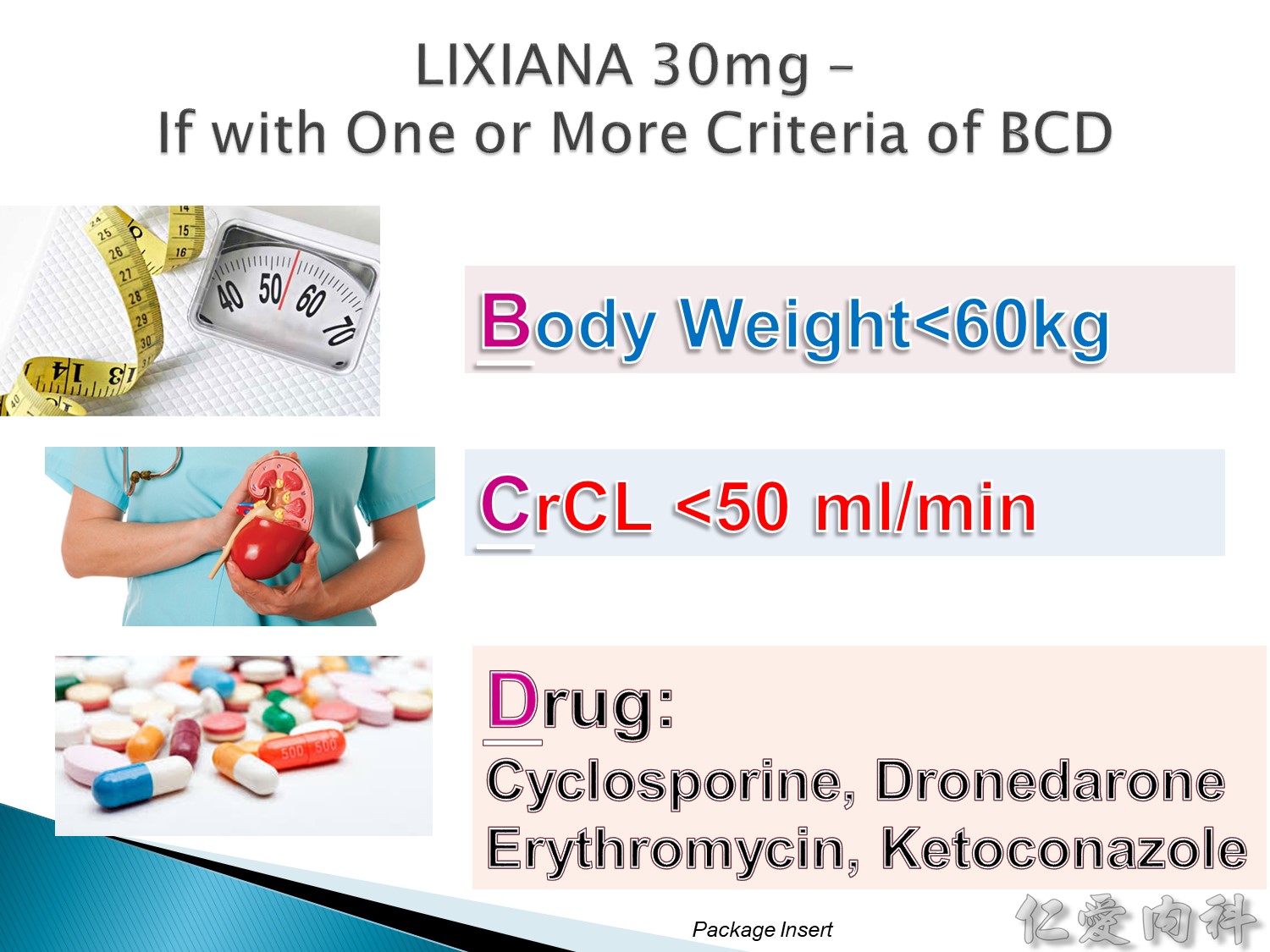
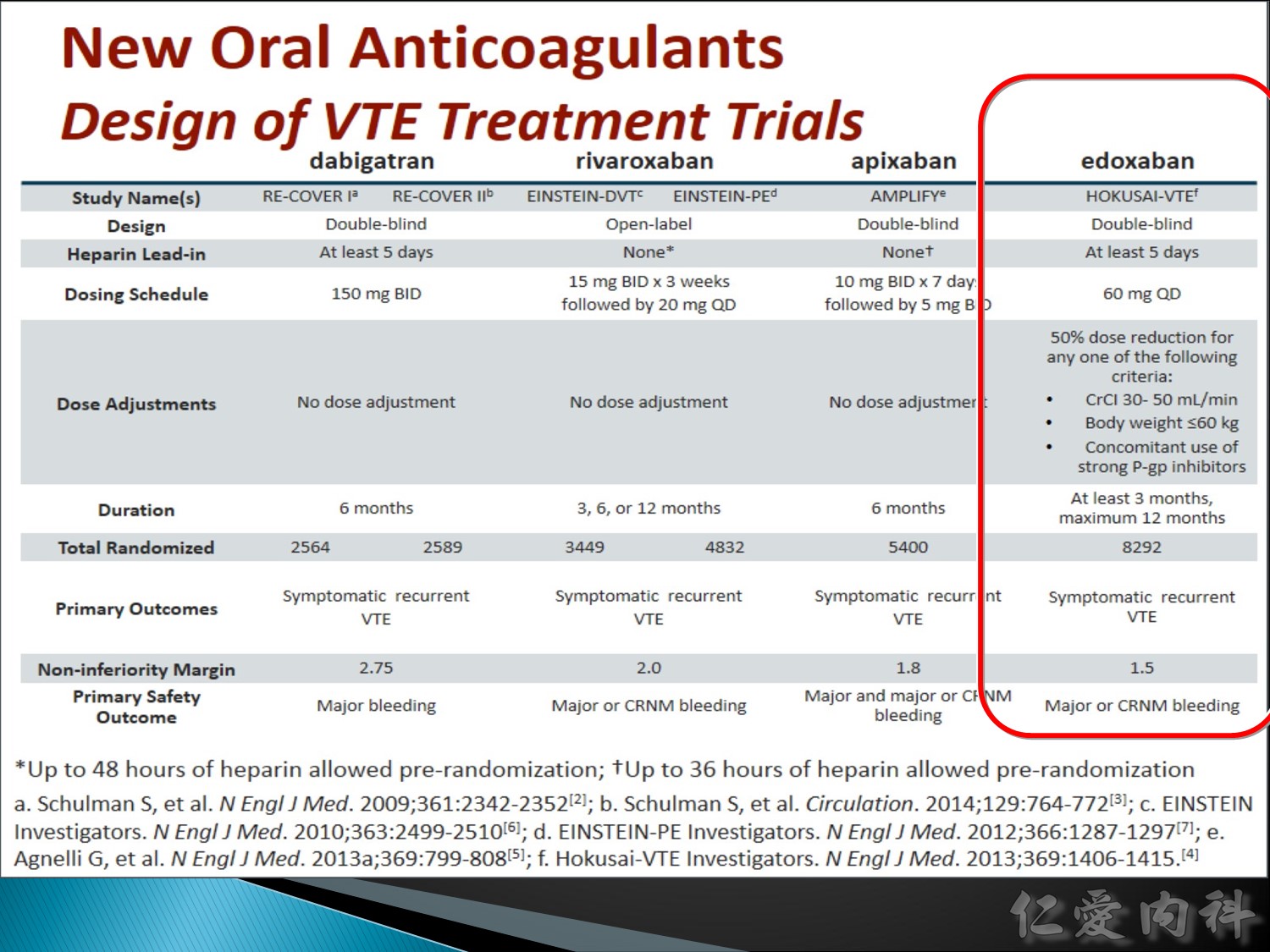
Low dose:腎功能差,體重較輕、有吃一些會有 interaction 的藥物的時候,在30/15 mg 這組就吃 15 mg,在 60/30 這組就吃 30 mg。
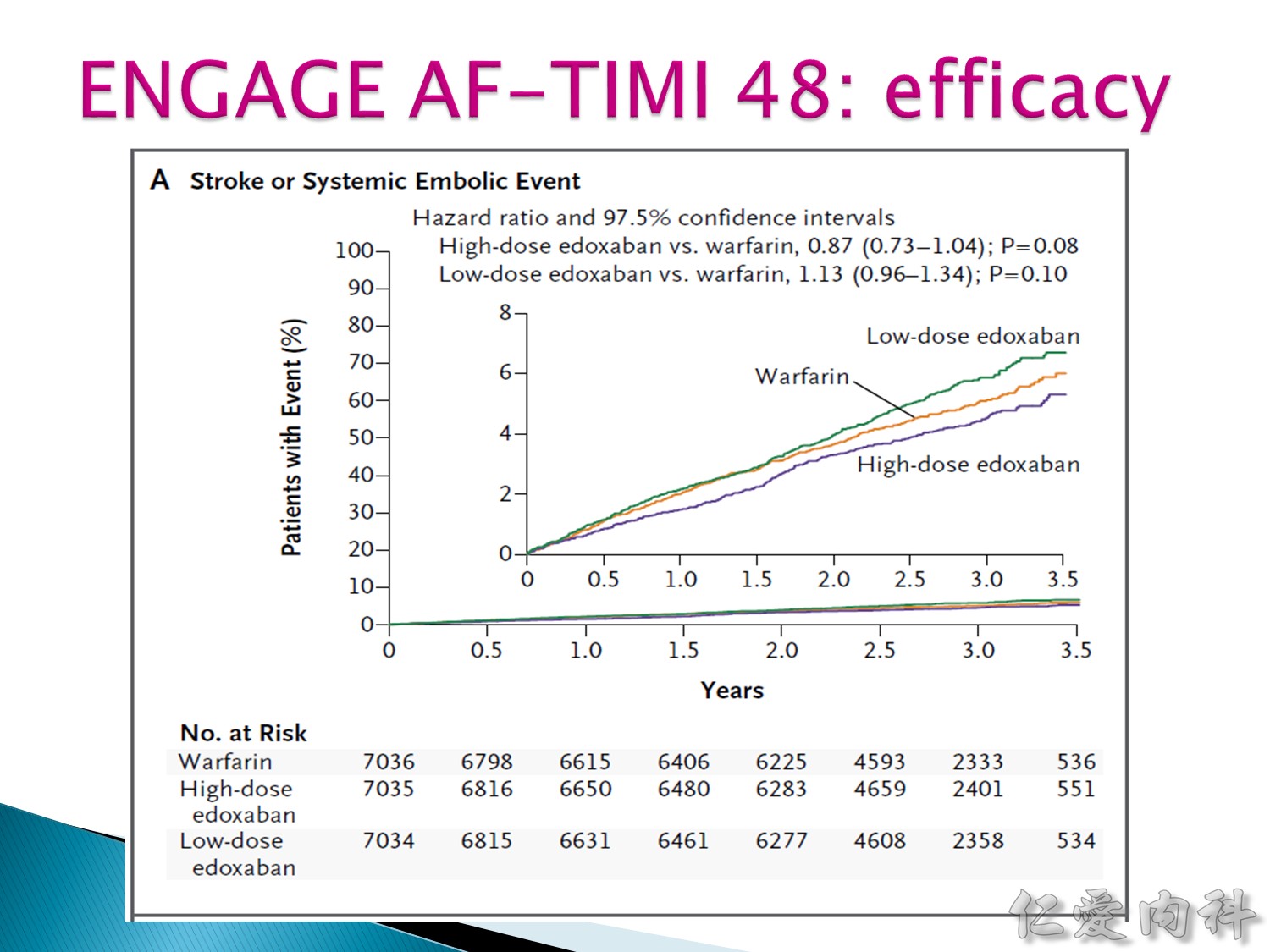
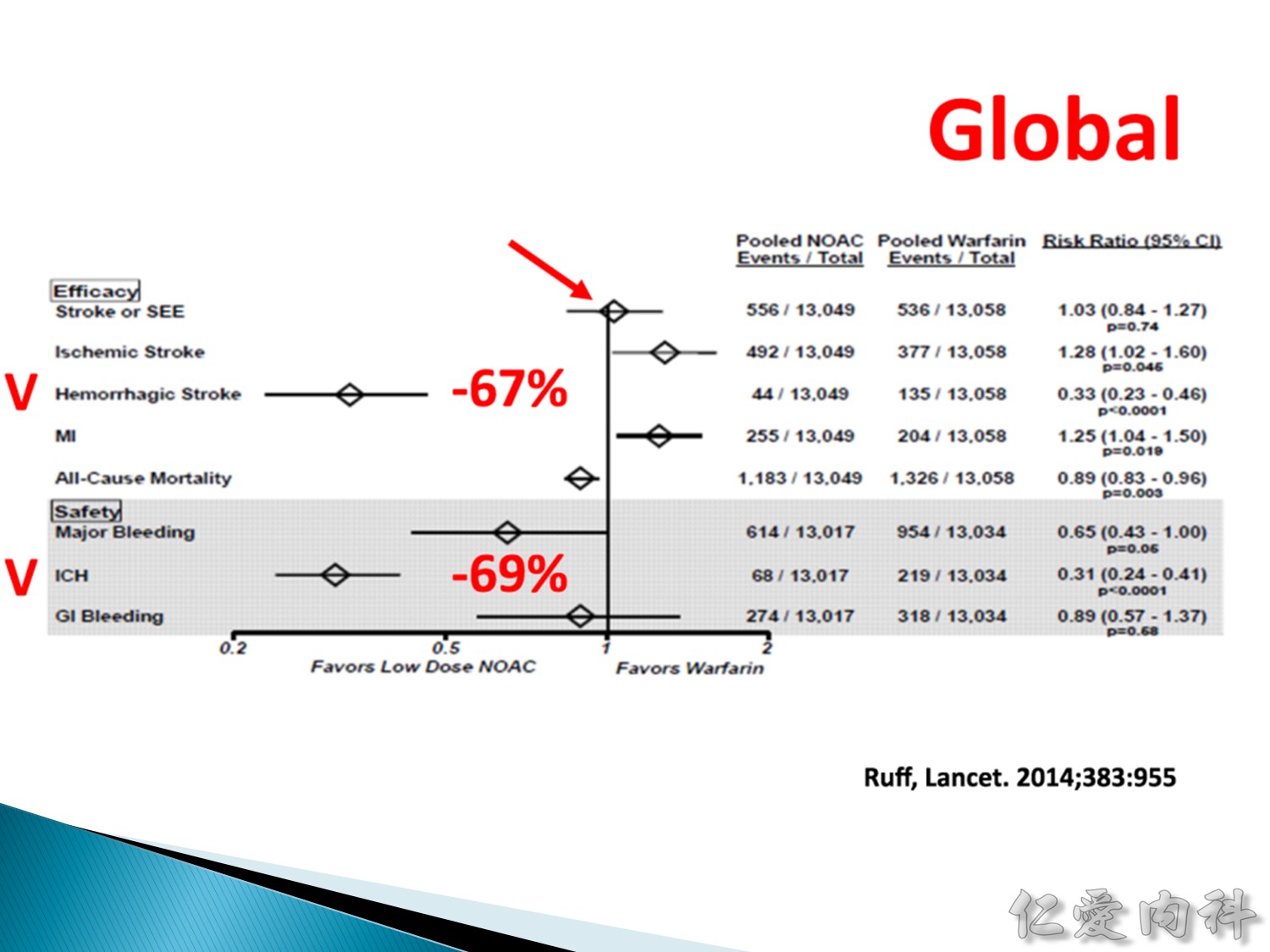
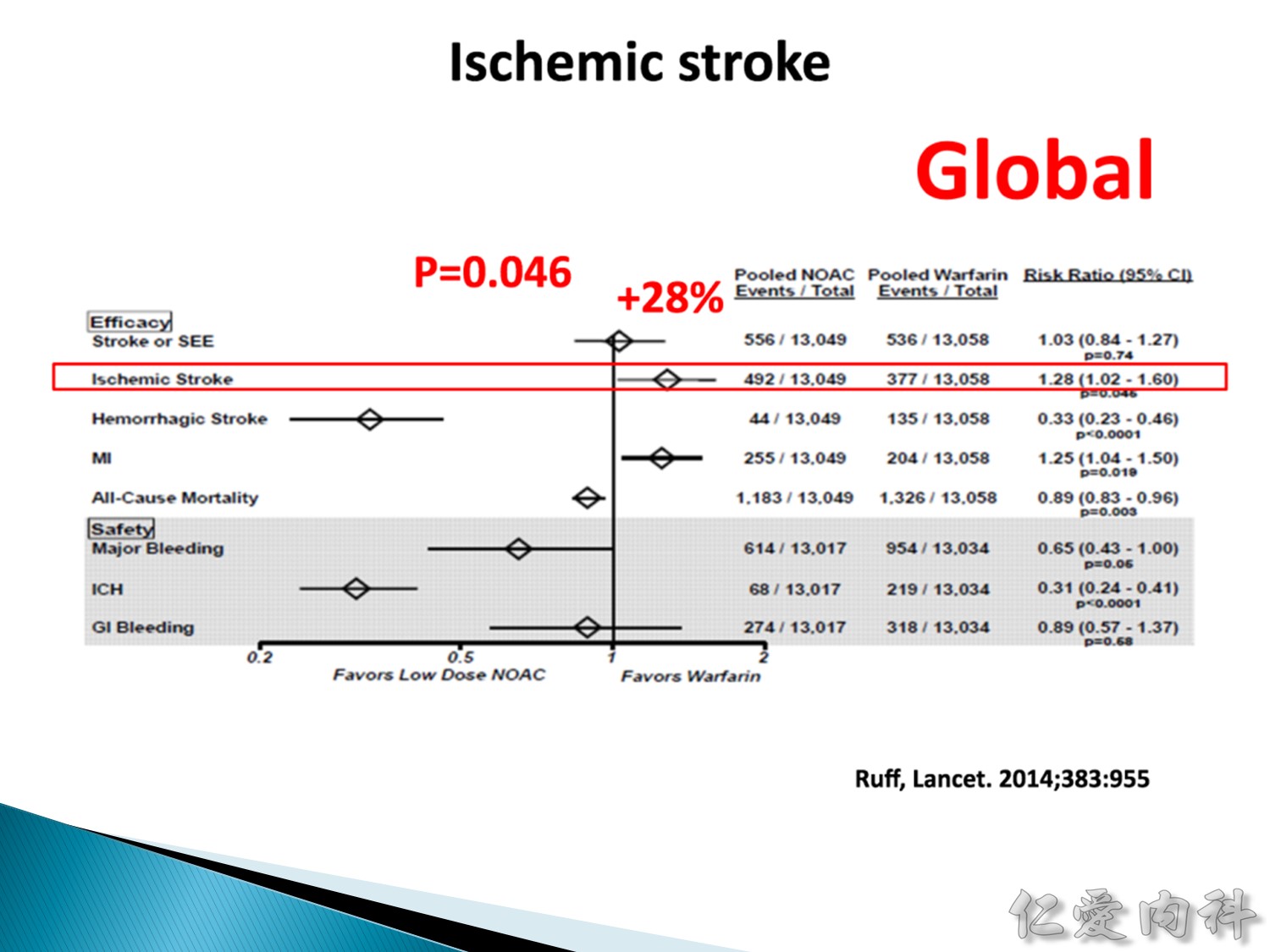
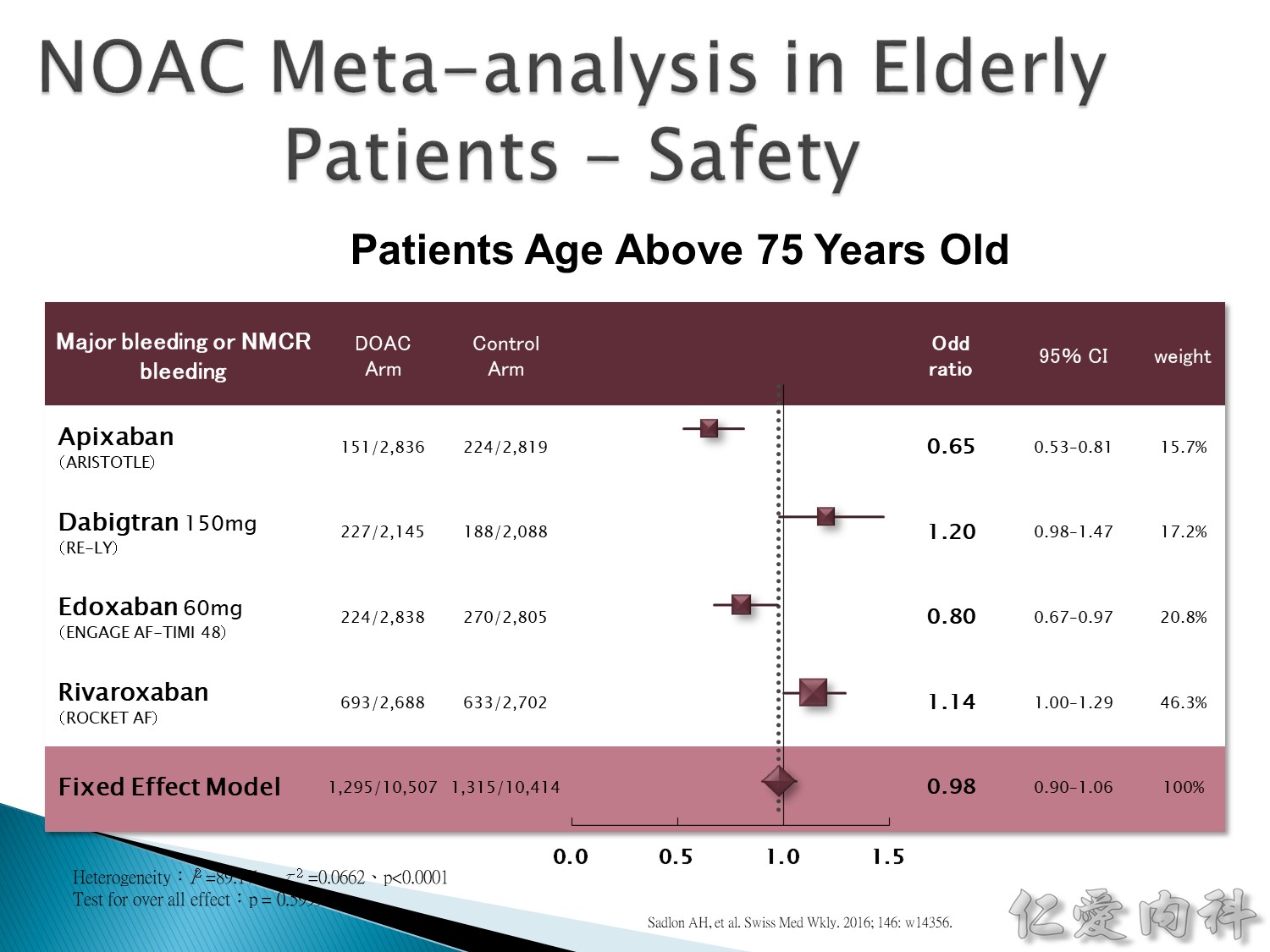
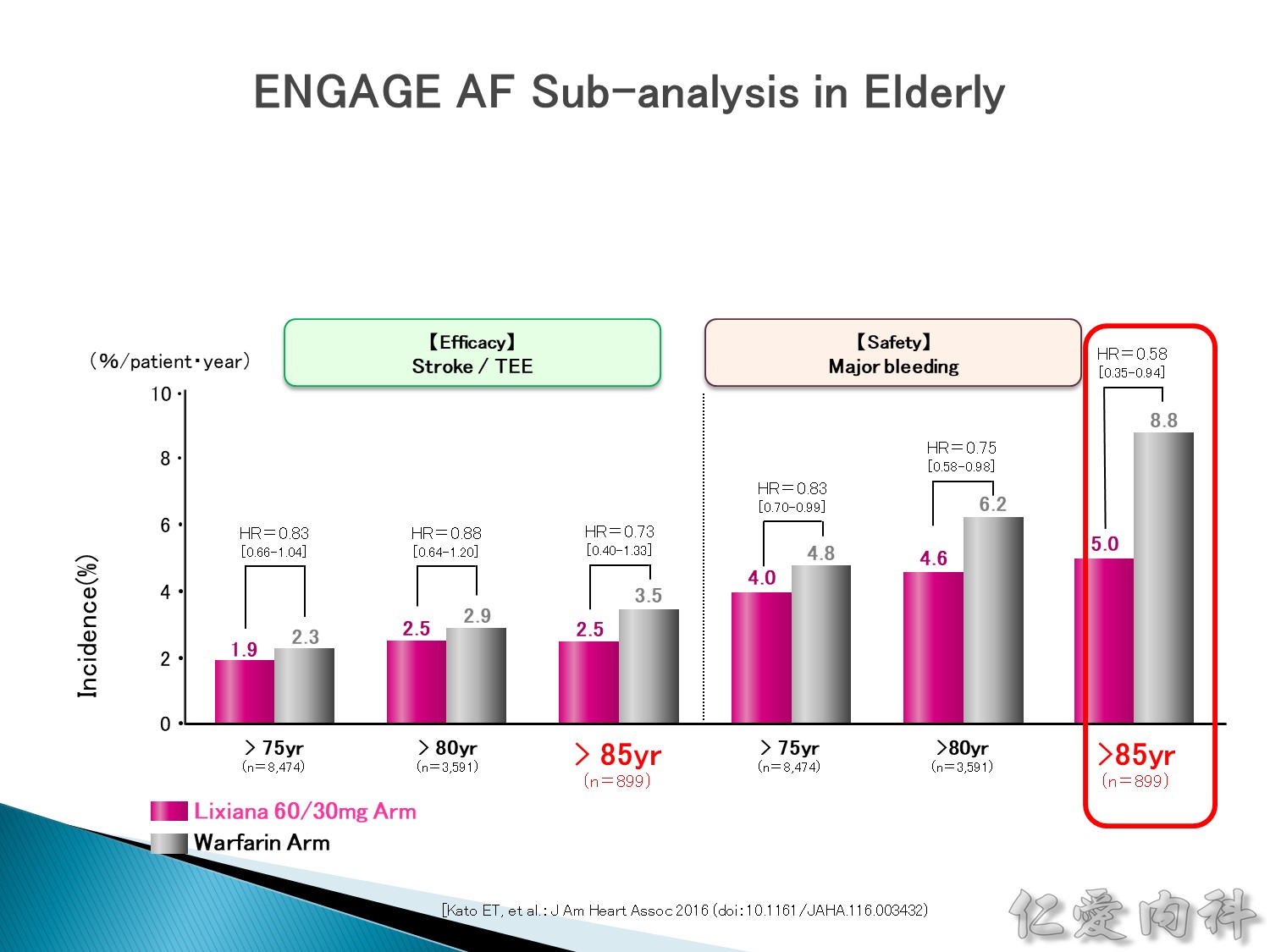
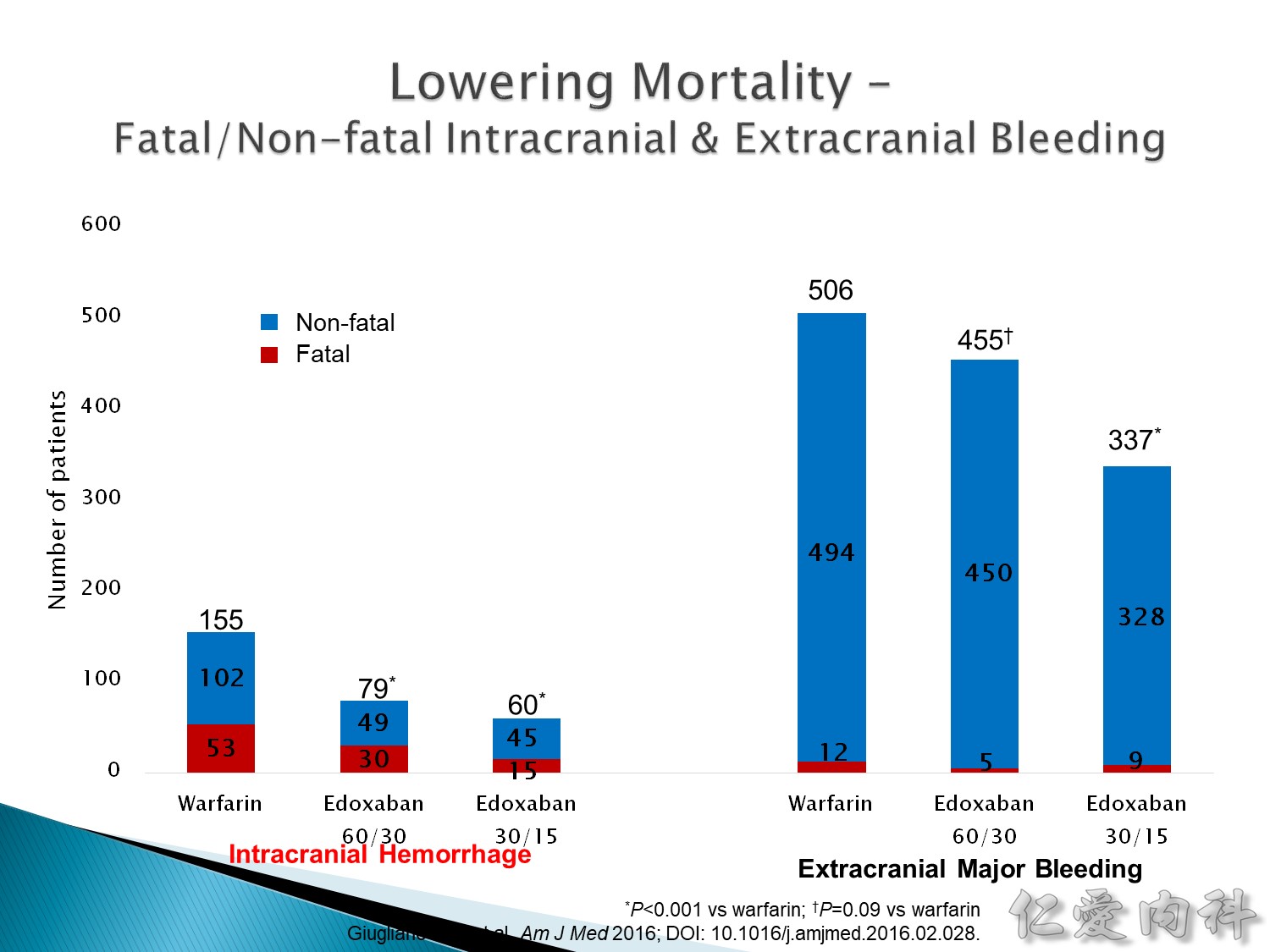
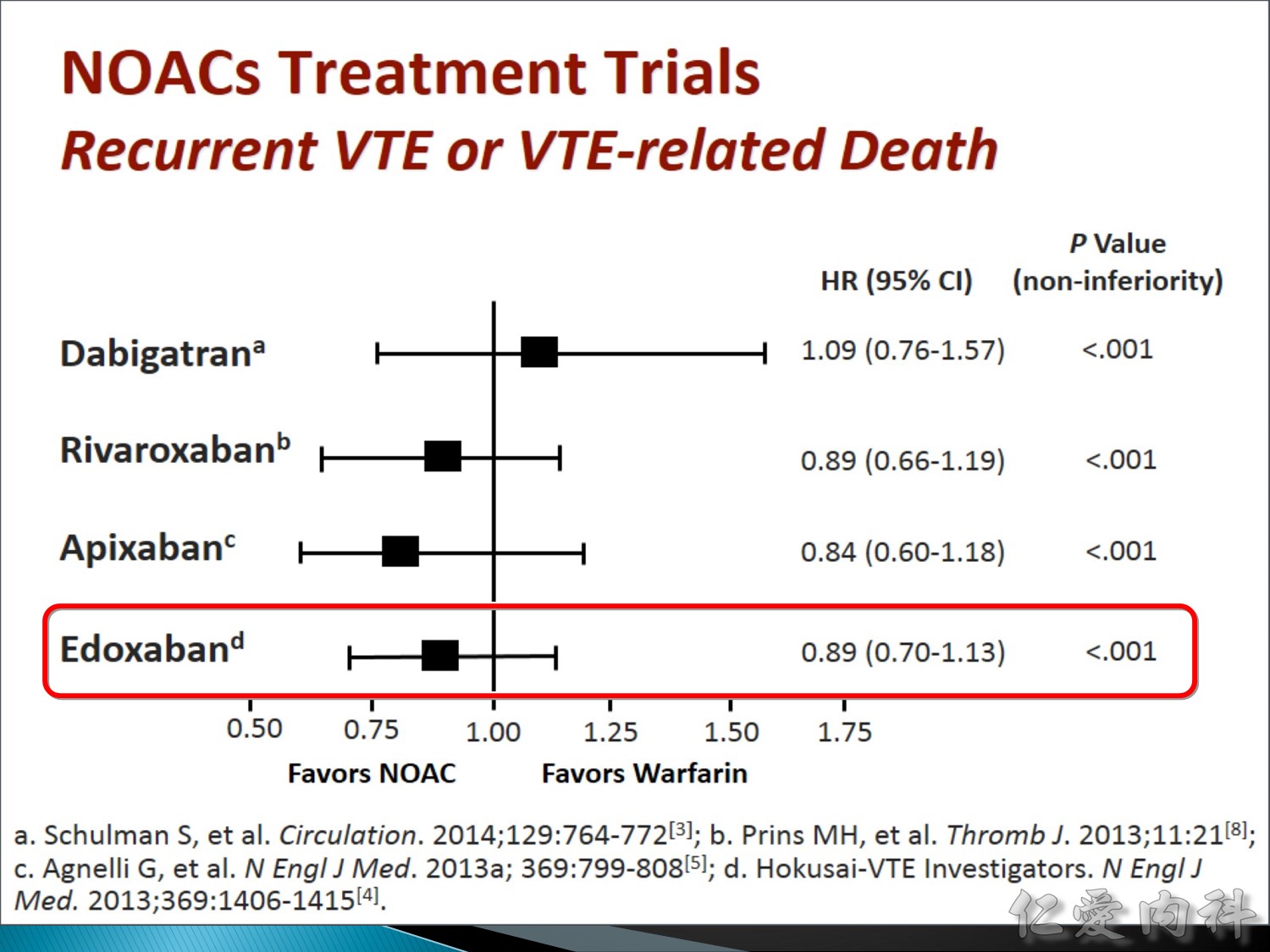
Edoxaban: high-dose (標準 dose 紫線) 的效果比 warfarin (黃線) 好,low-dose 比warfarin 效果差。
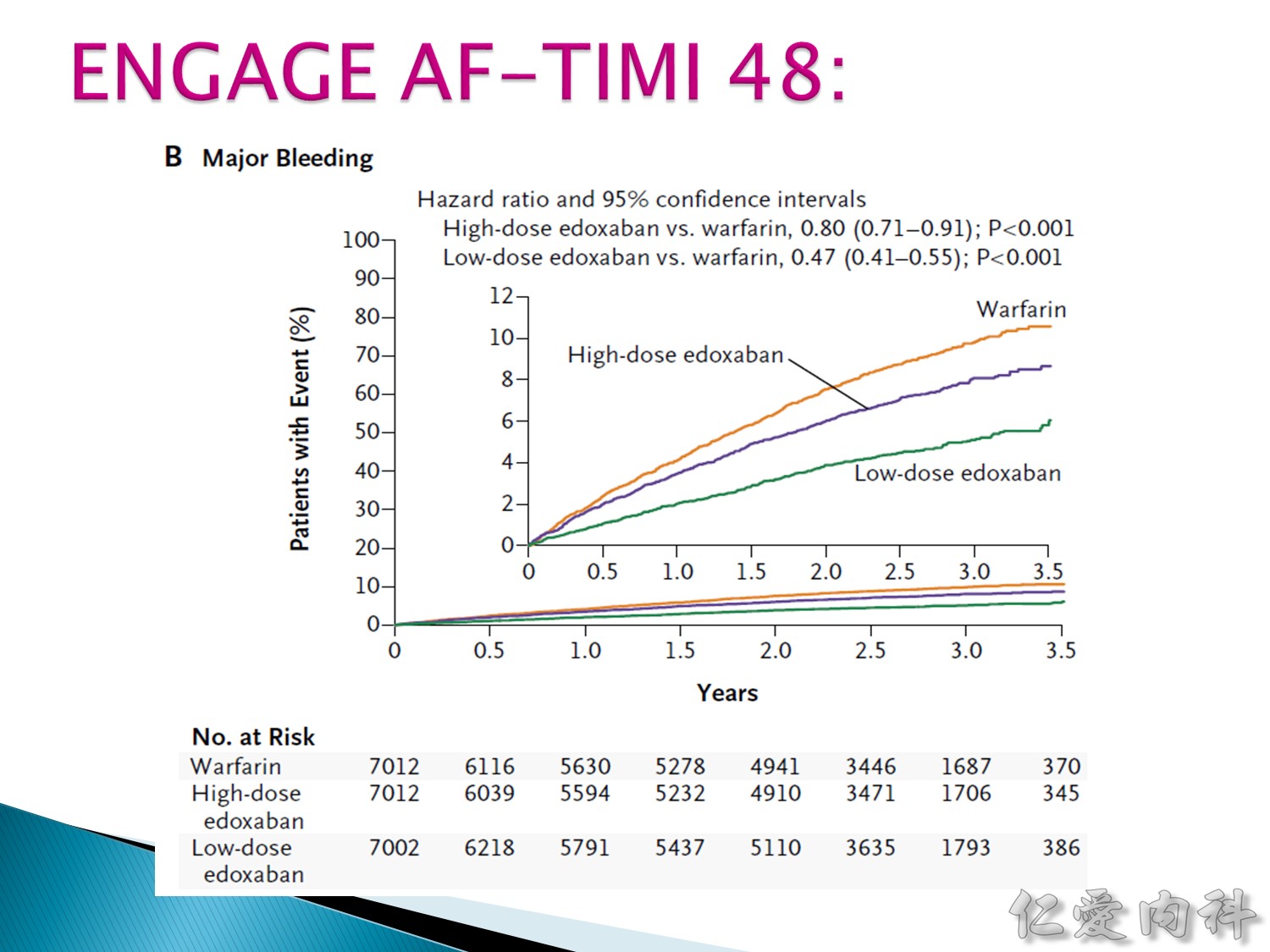
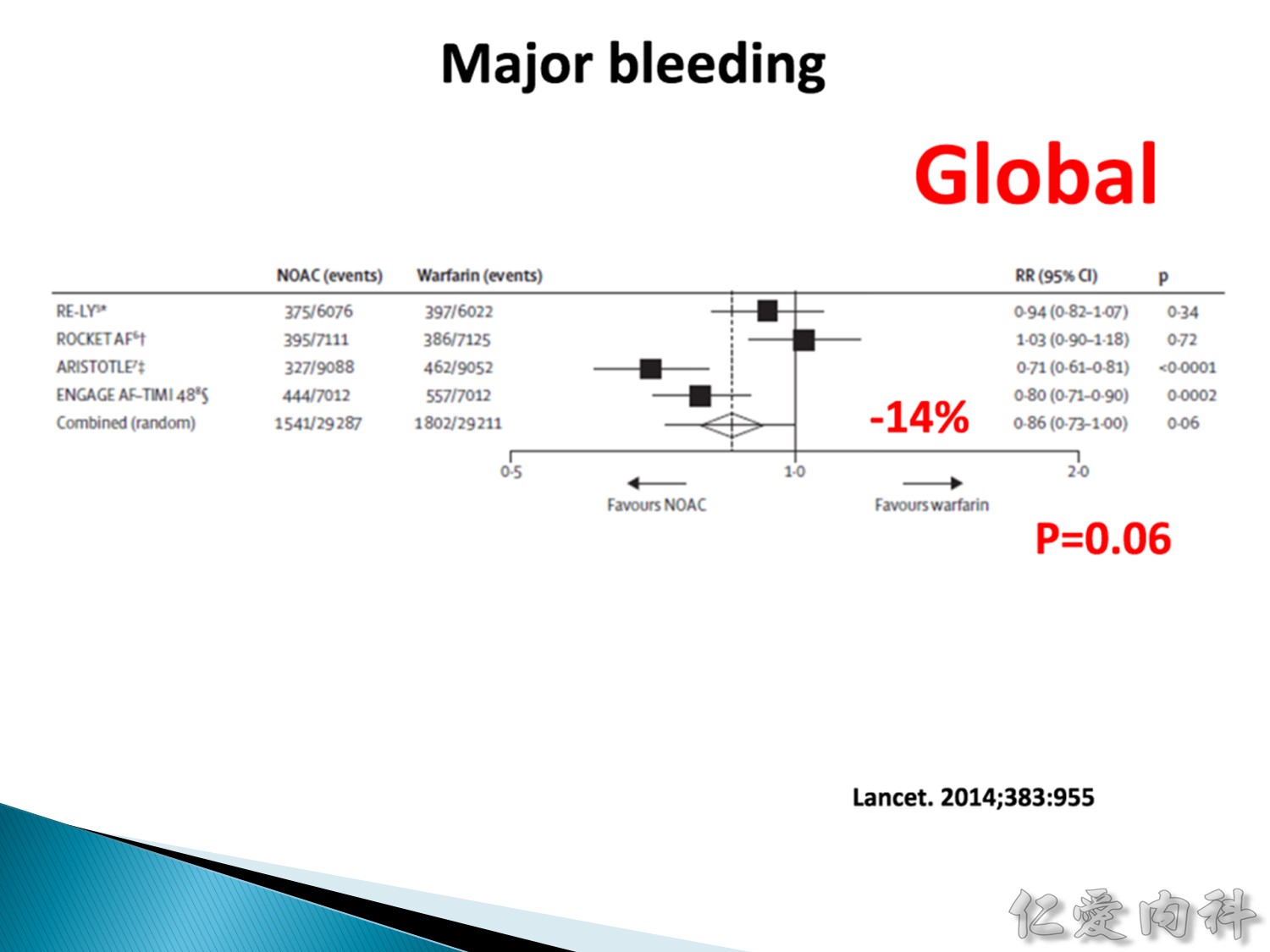
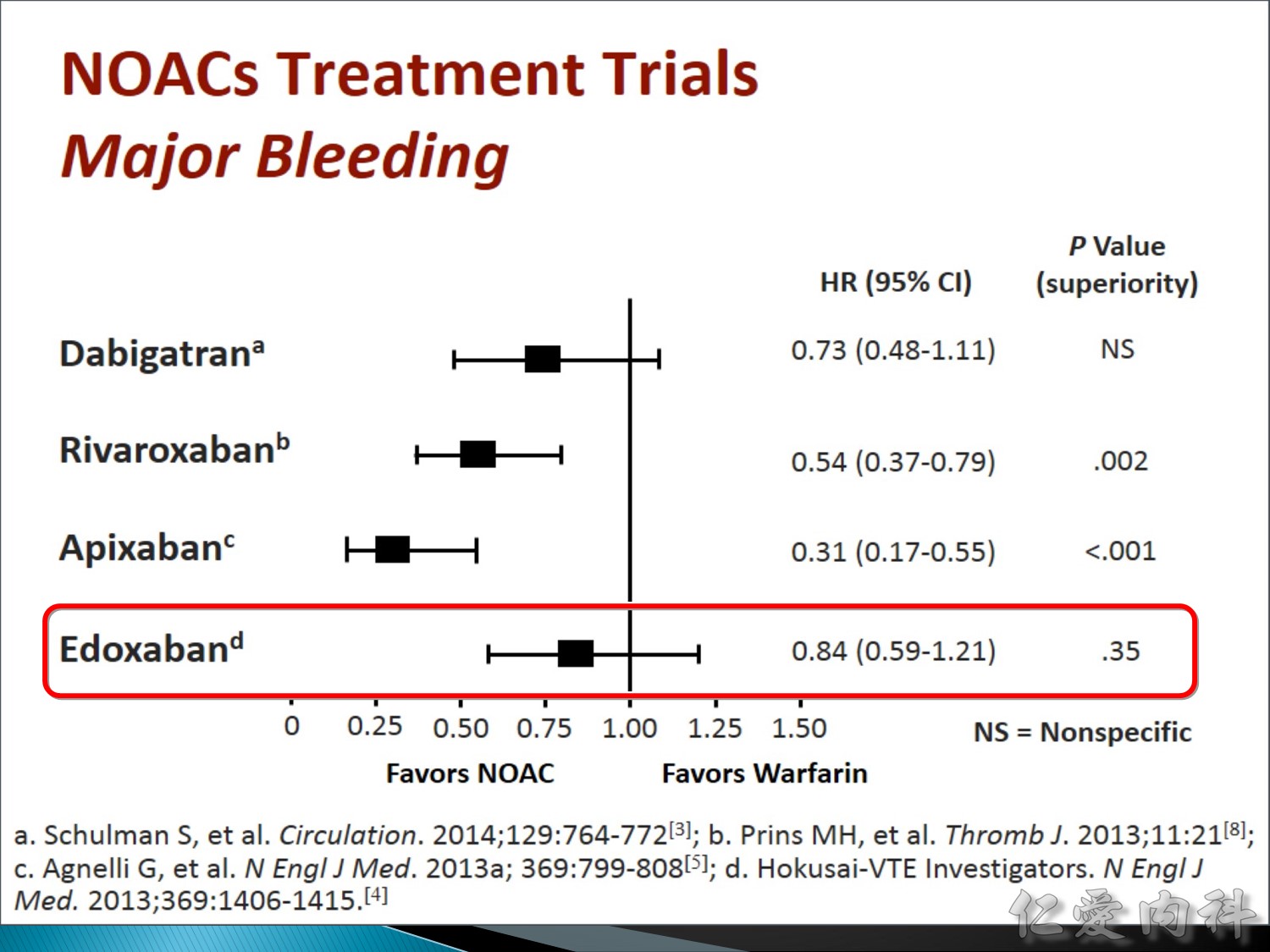
Major bleeding warfarin 比 edoxaban 風險高。
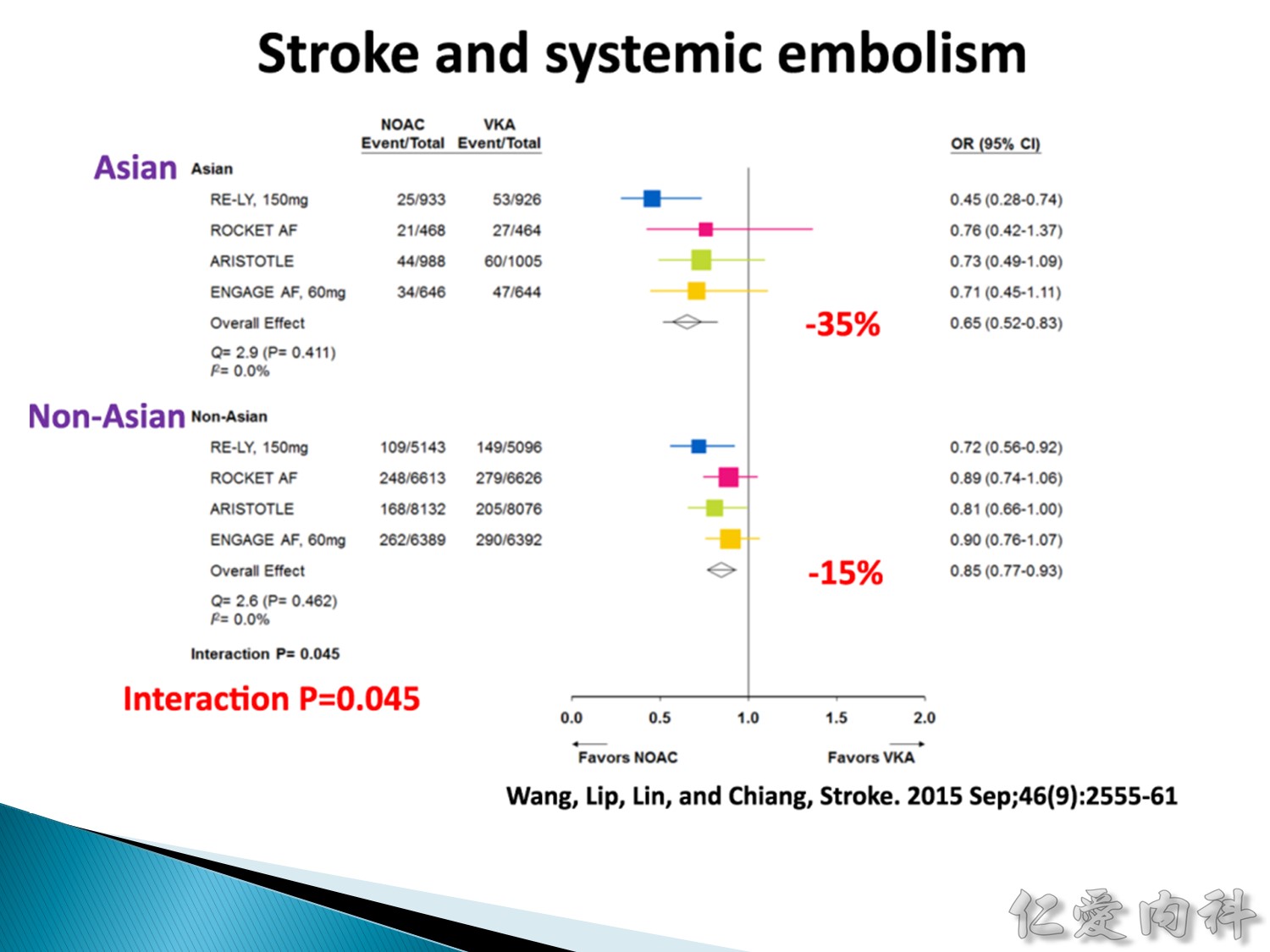
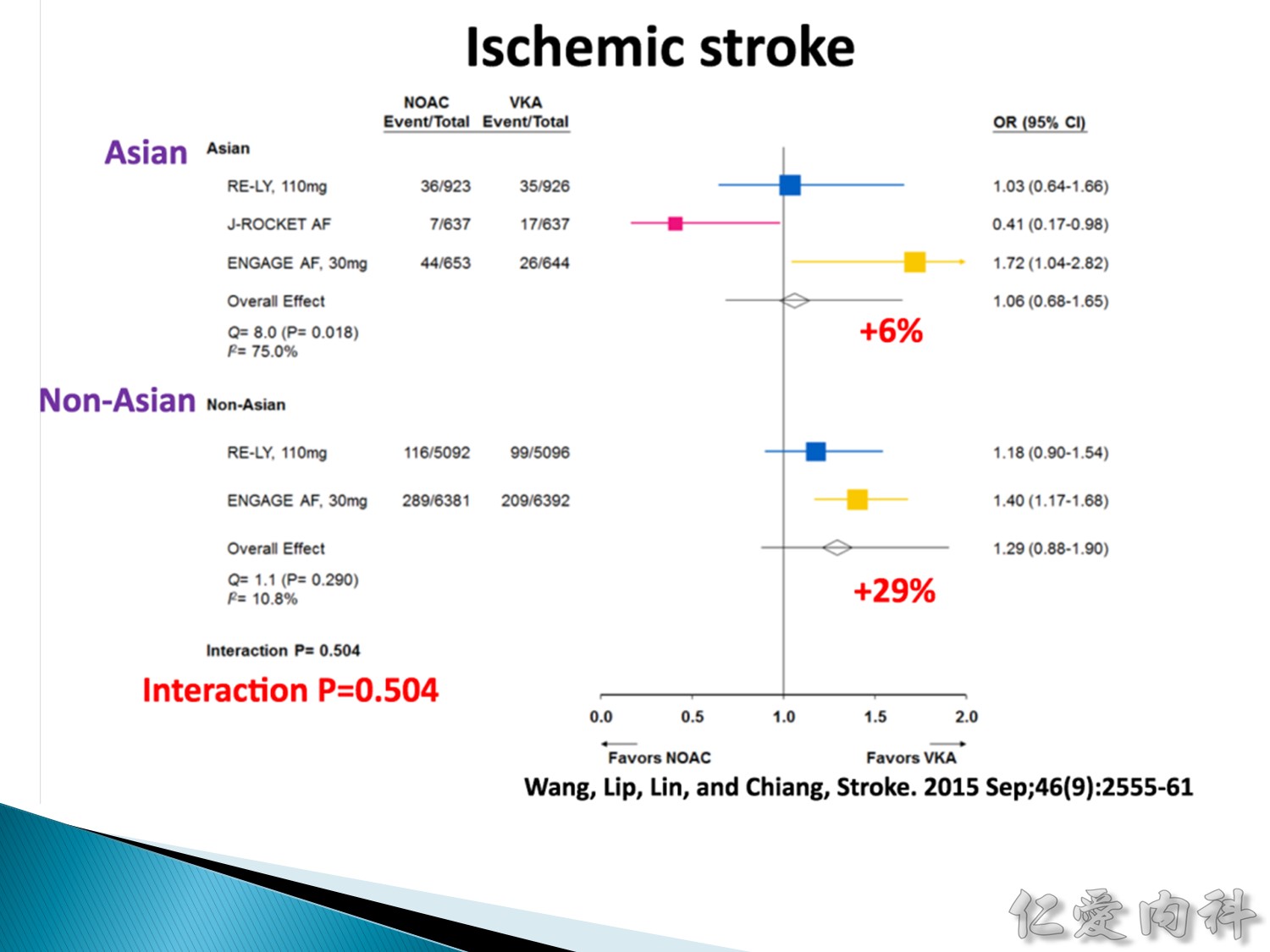
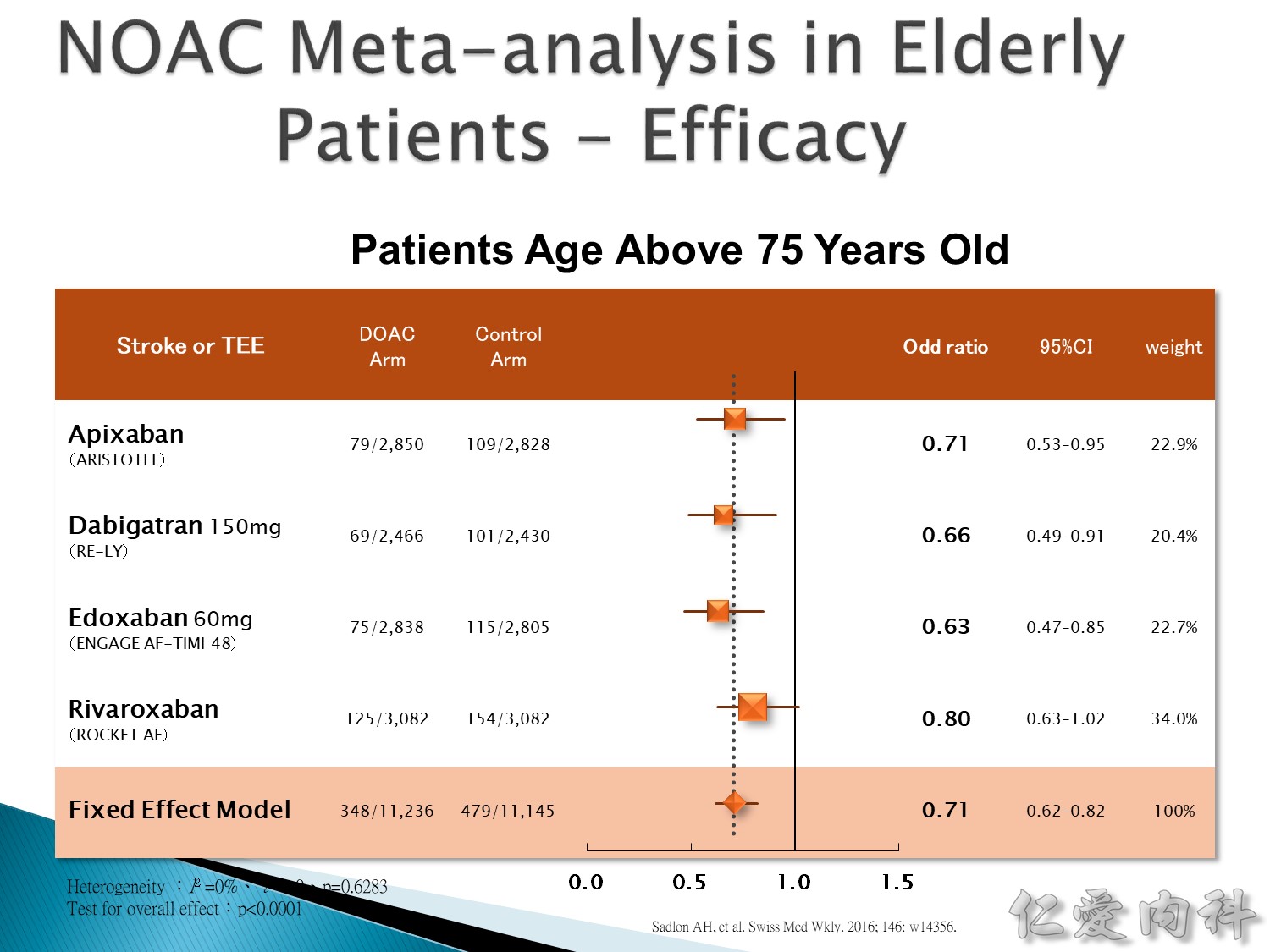
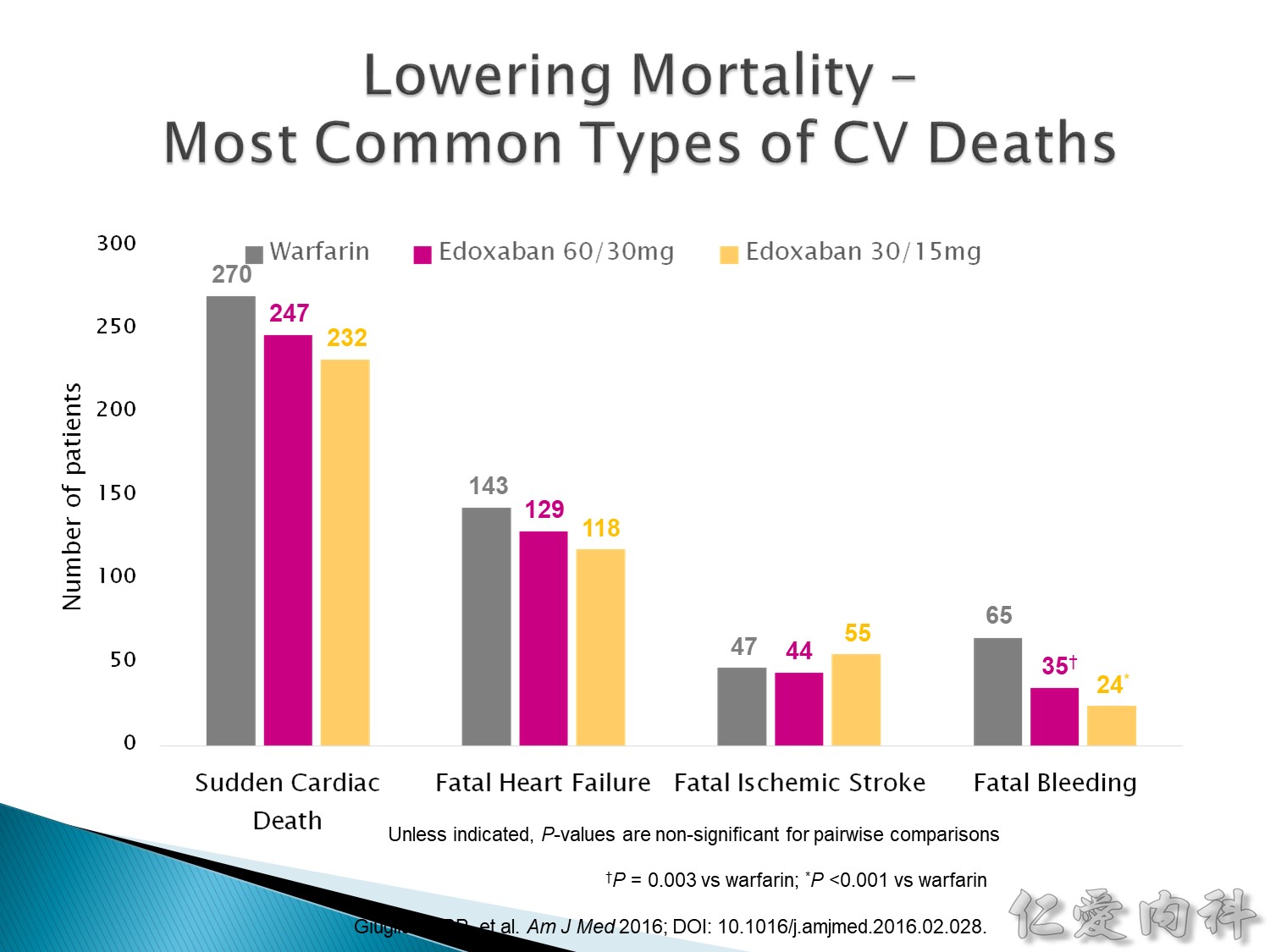
NOAC 保護效果在 Asian 的 ischemia stroke 減少比例可達 35%,non-Asian ischemia stroke 則只有減少 15%。
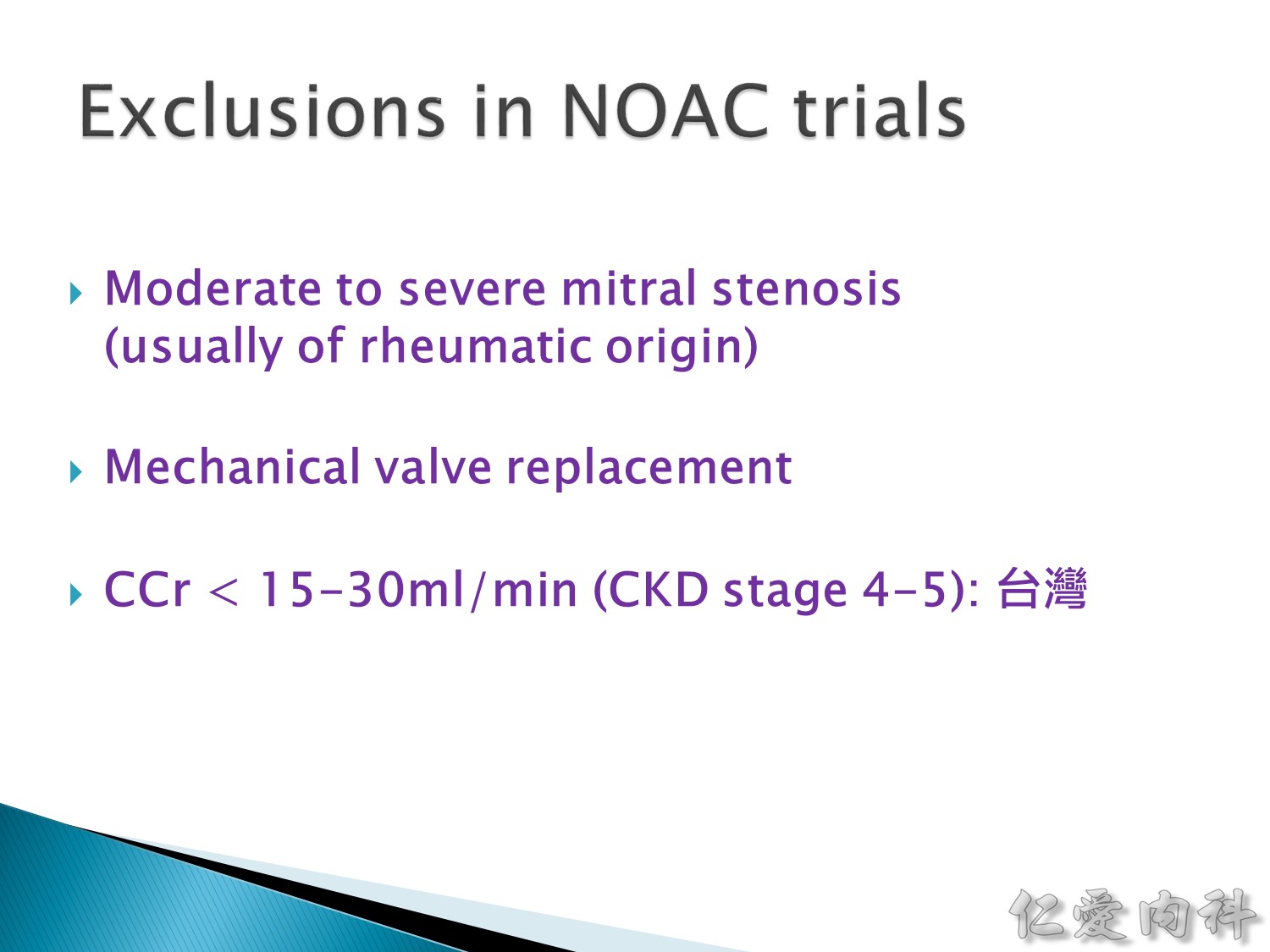
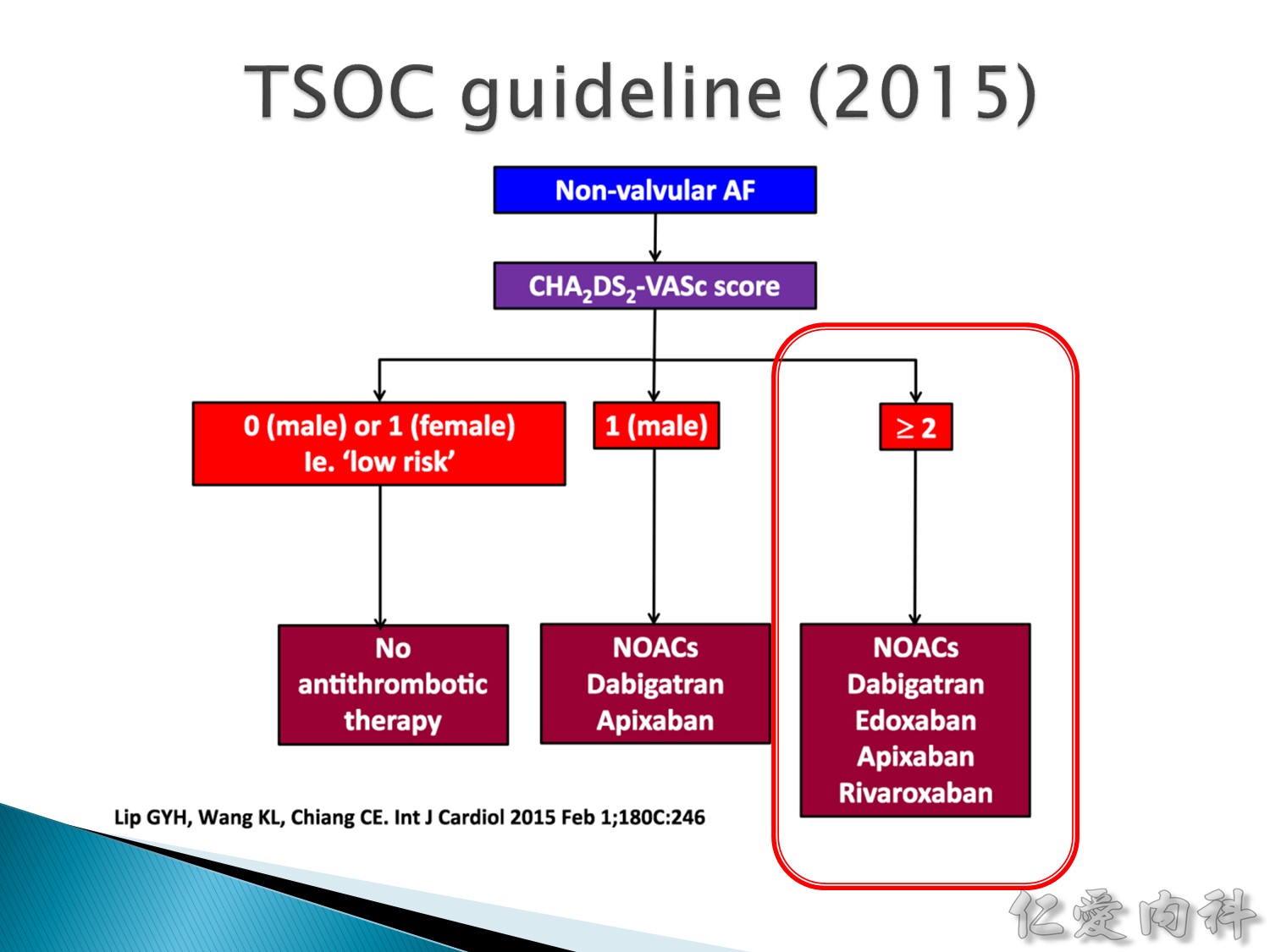
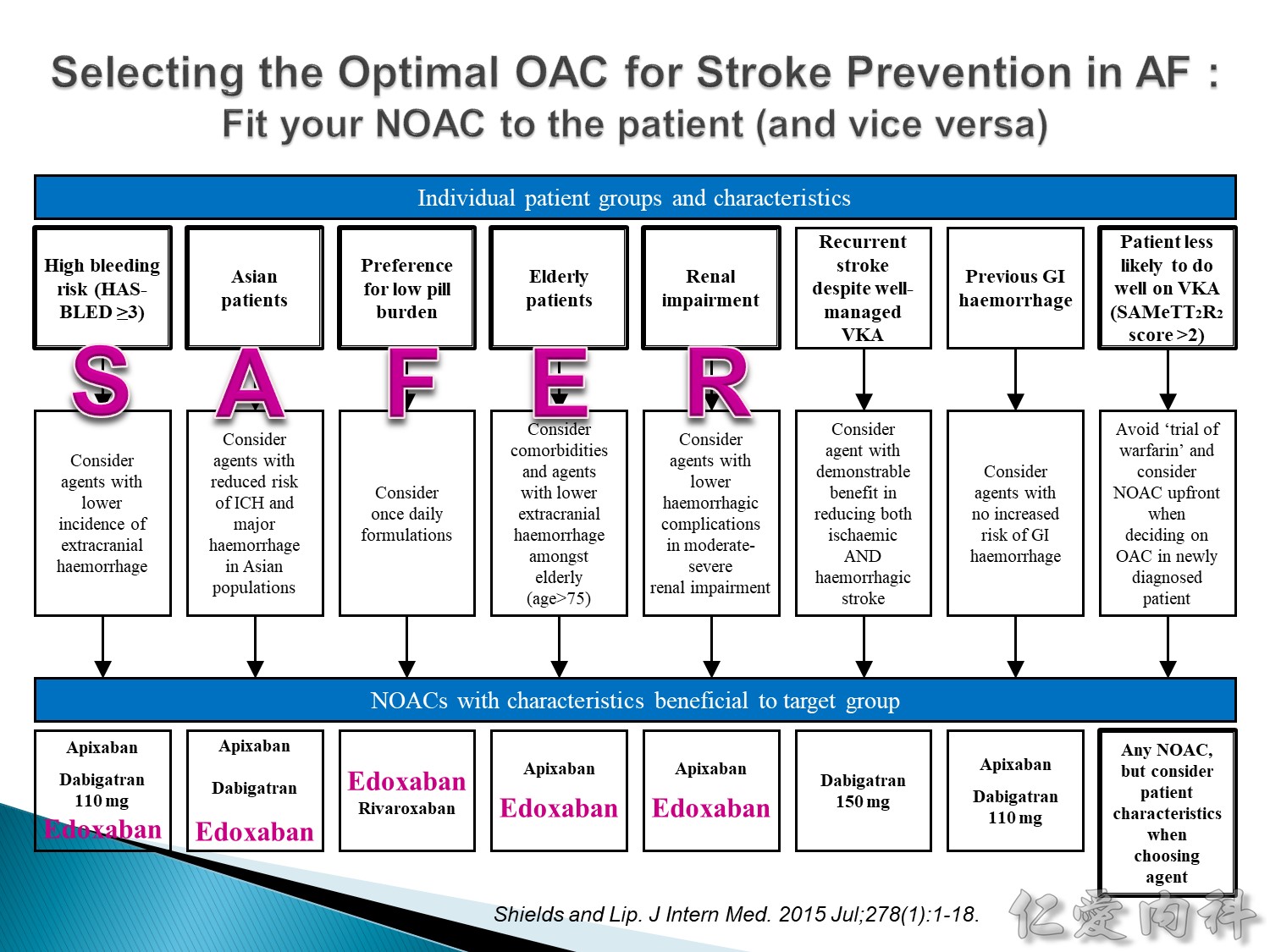
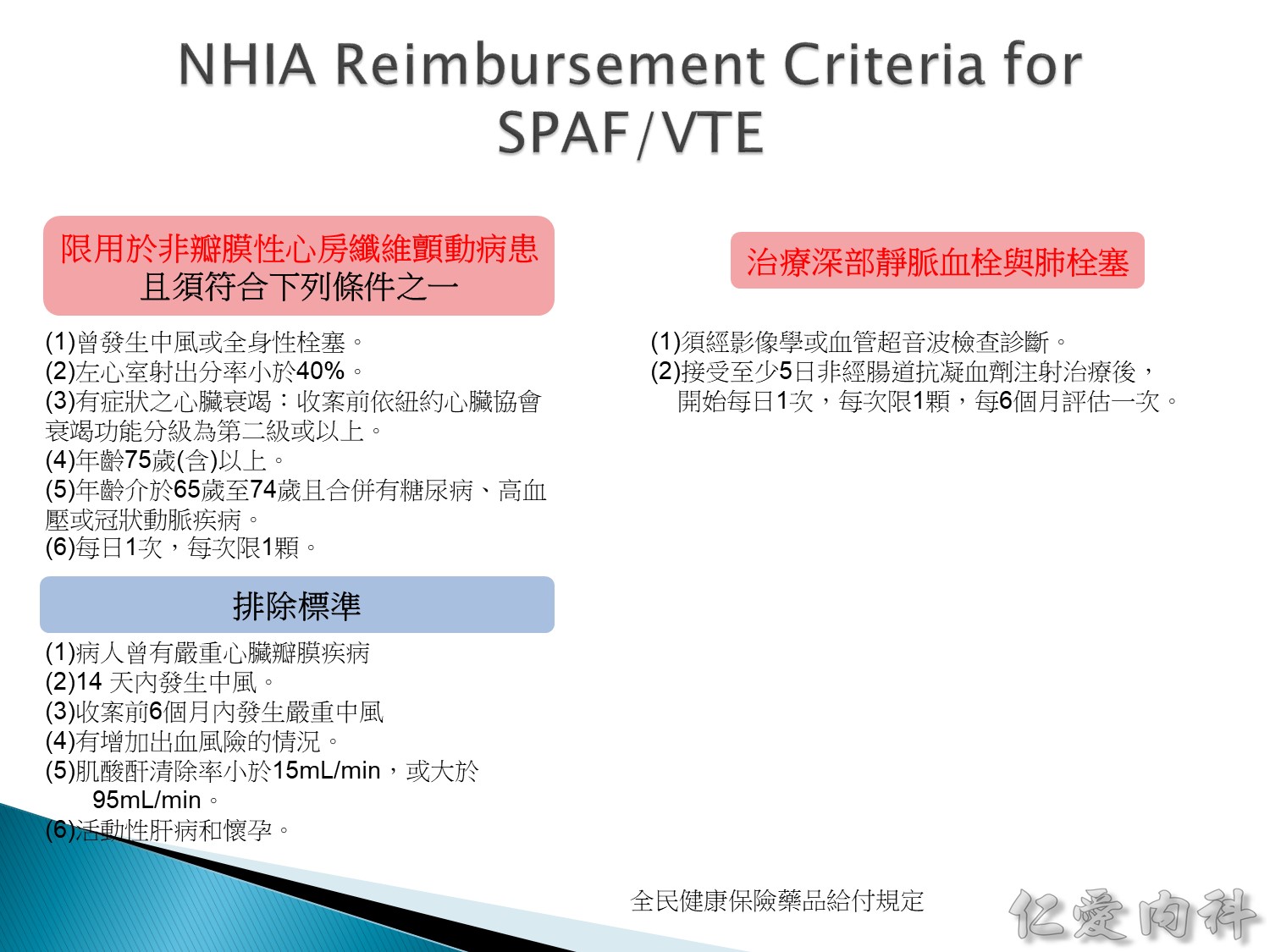
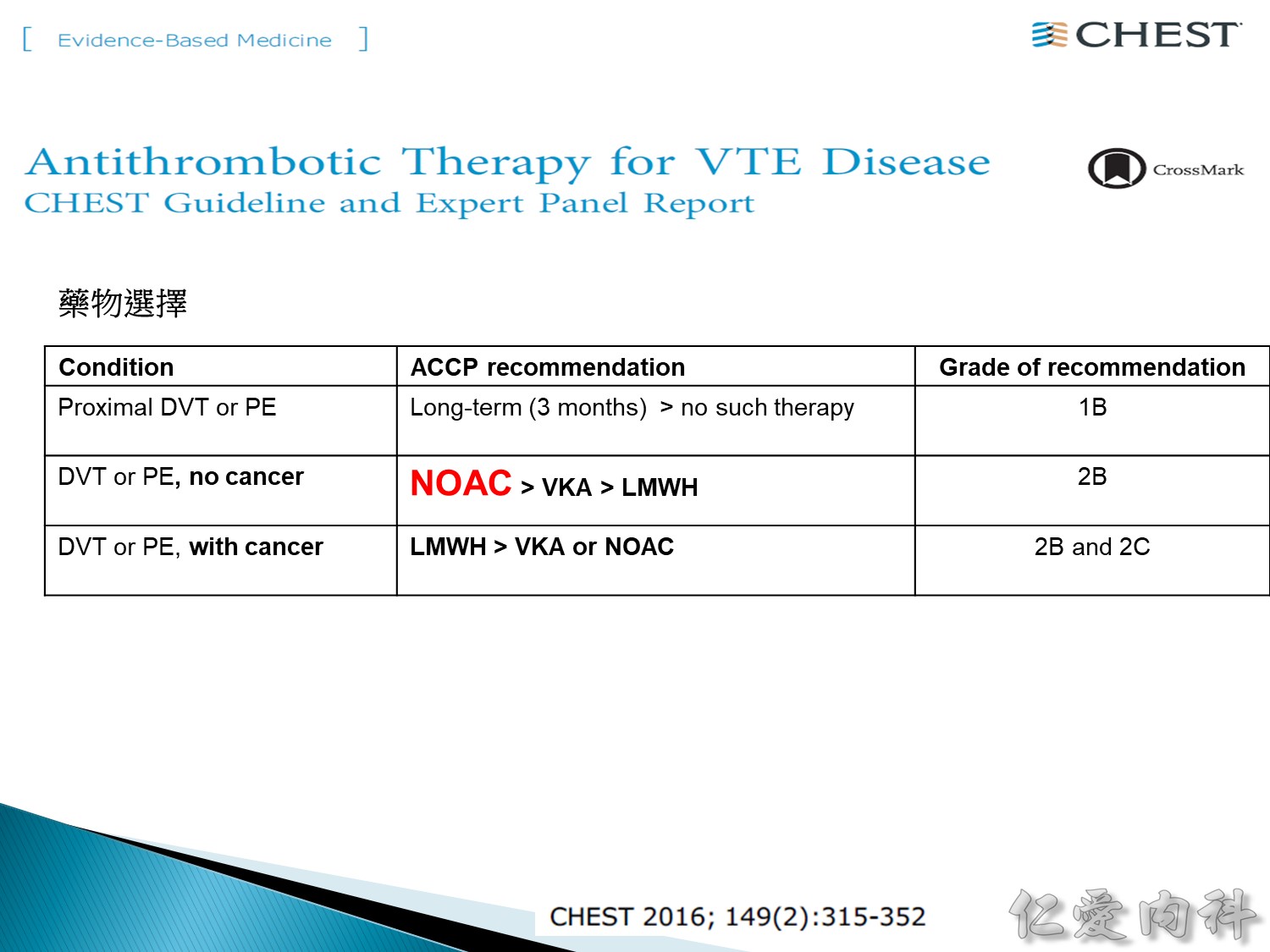
NOAC 有三個族群不能用:
1. rhumatic heart 造成的 MS (moderate to severe) 不能用 (mild可以用)
2. mechanical valve 不行 (因為不在 trial 裡面)
3. 腎功能 CCr<15 不行,CCr: 15-50 要減半用
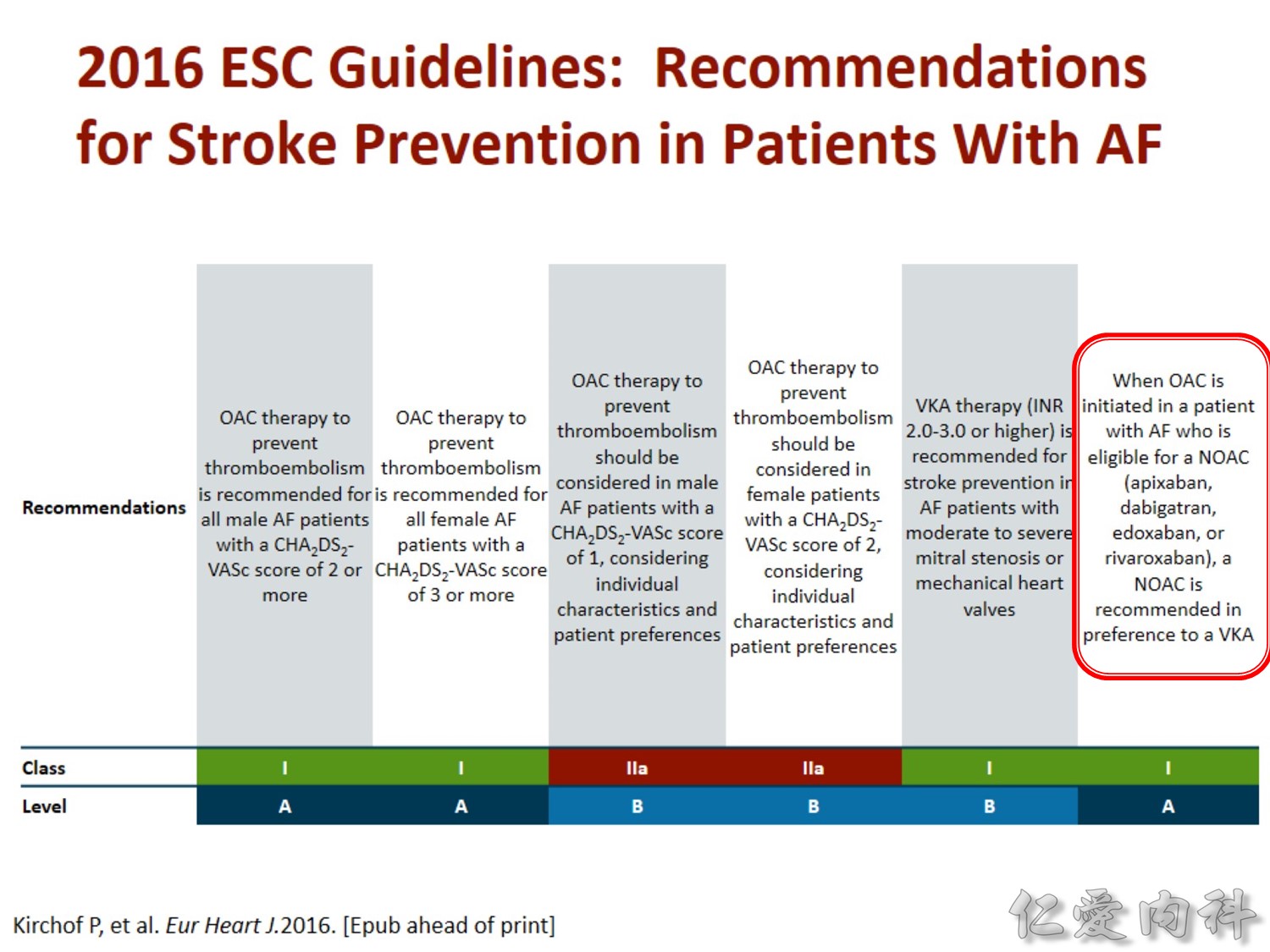
只要能用 NOAC 就應該用 NOAC。
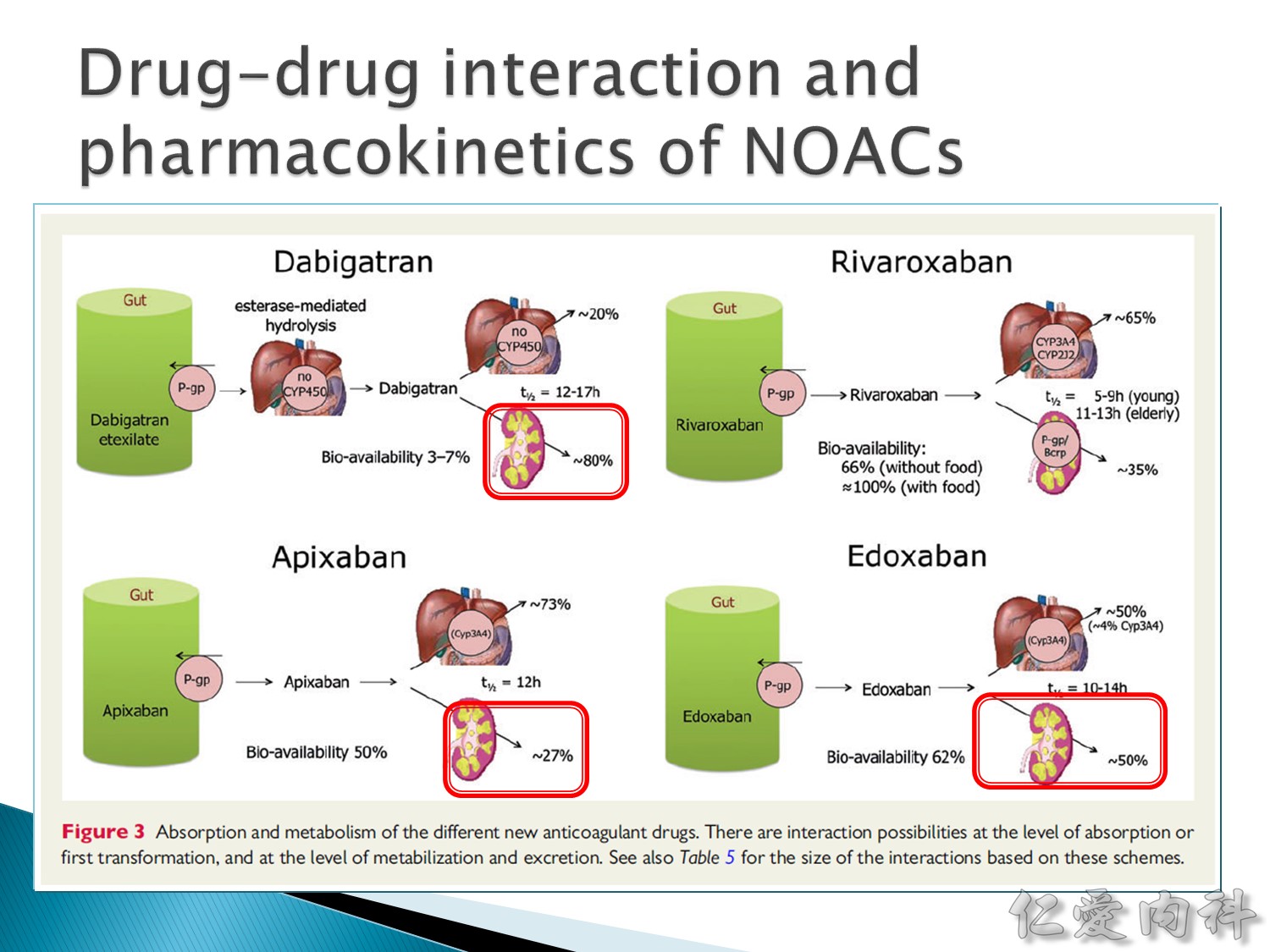
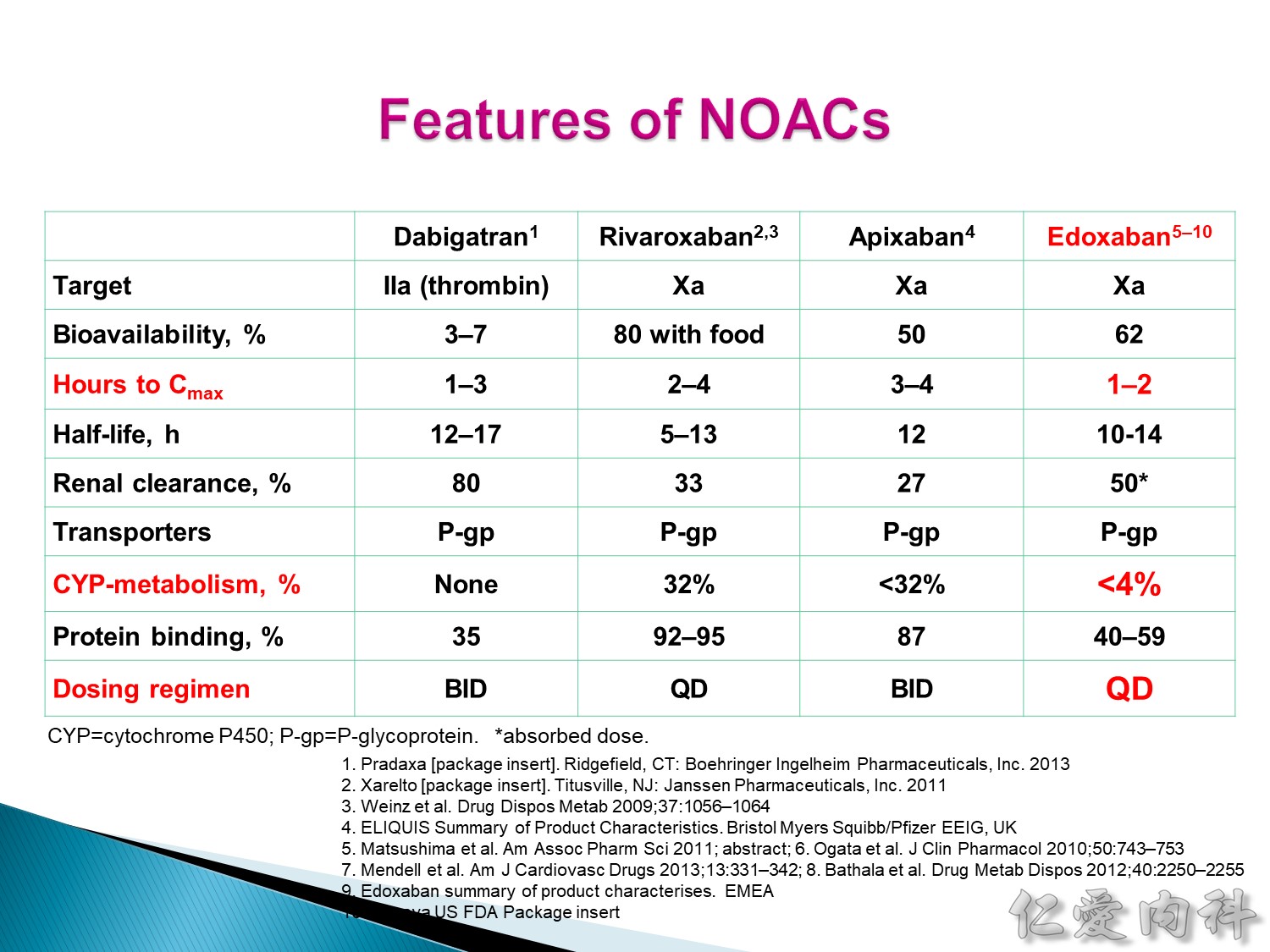
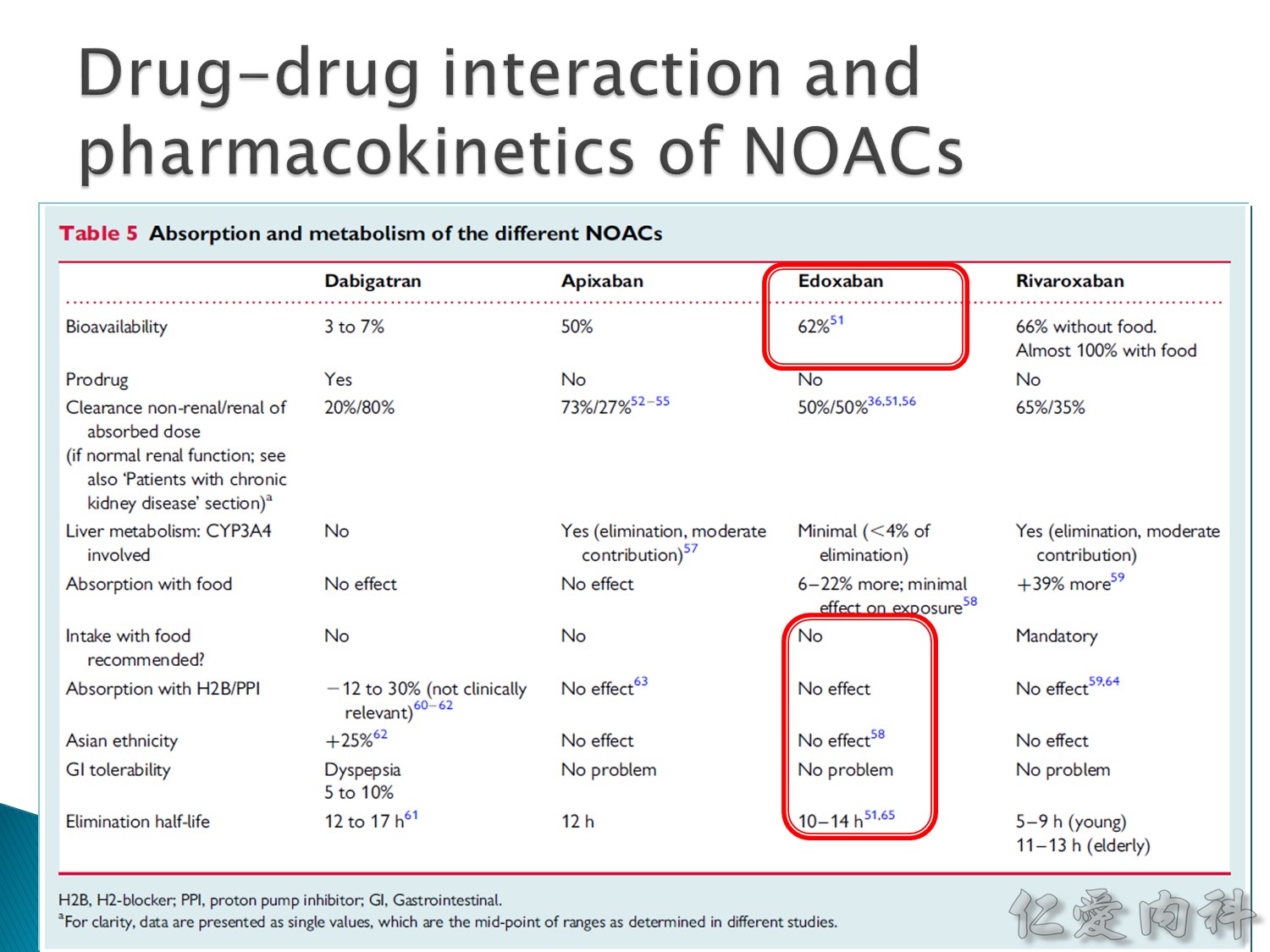
Rivaroxaben 一定要跟食物一起吃生體可用率才是 100%。
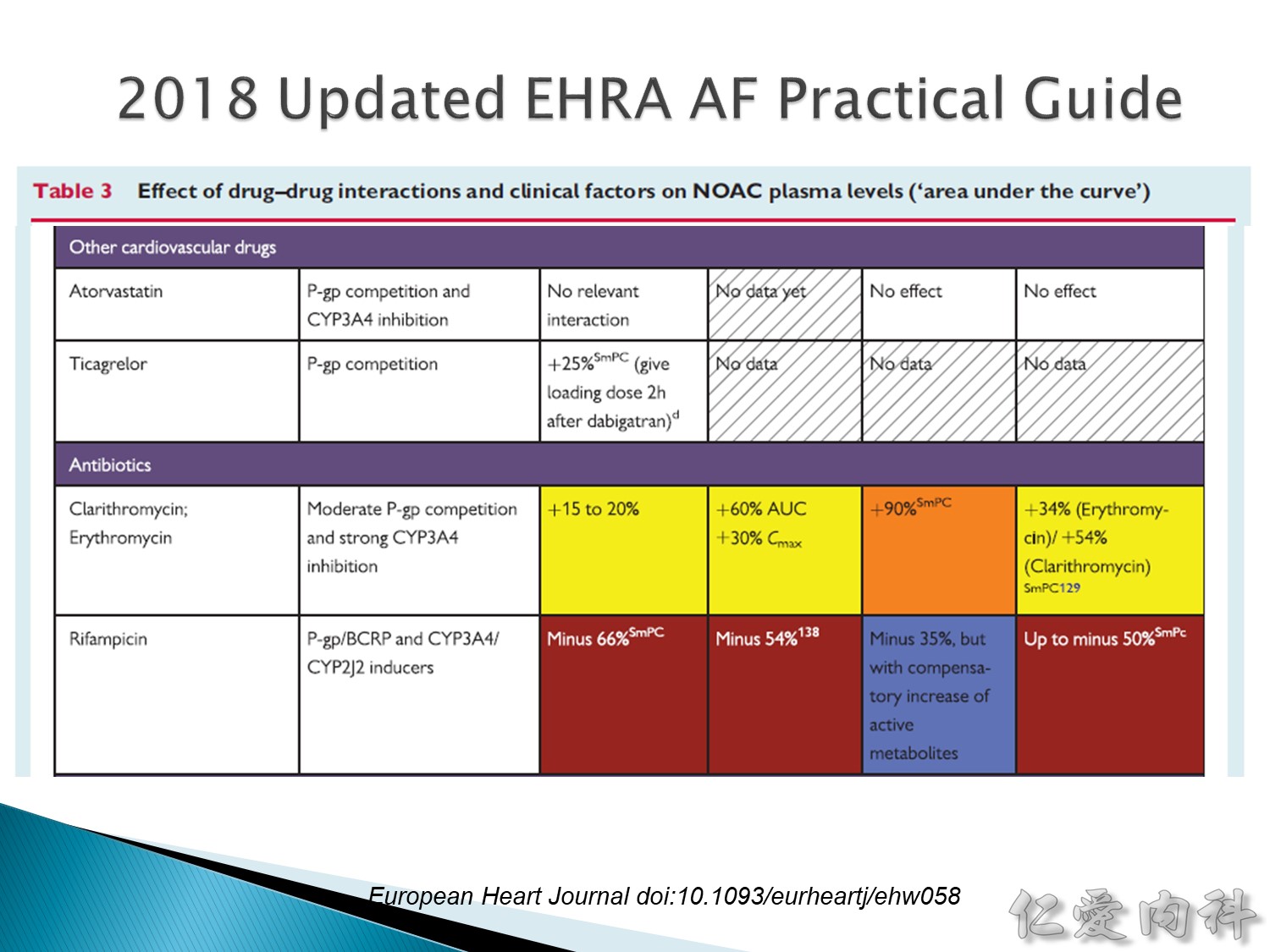
Edoxaban 和藥物交互作用最少。
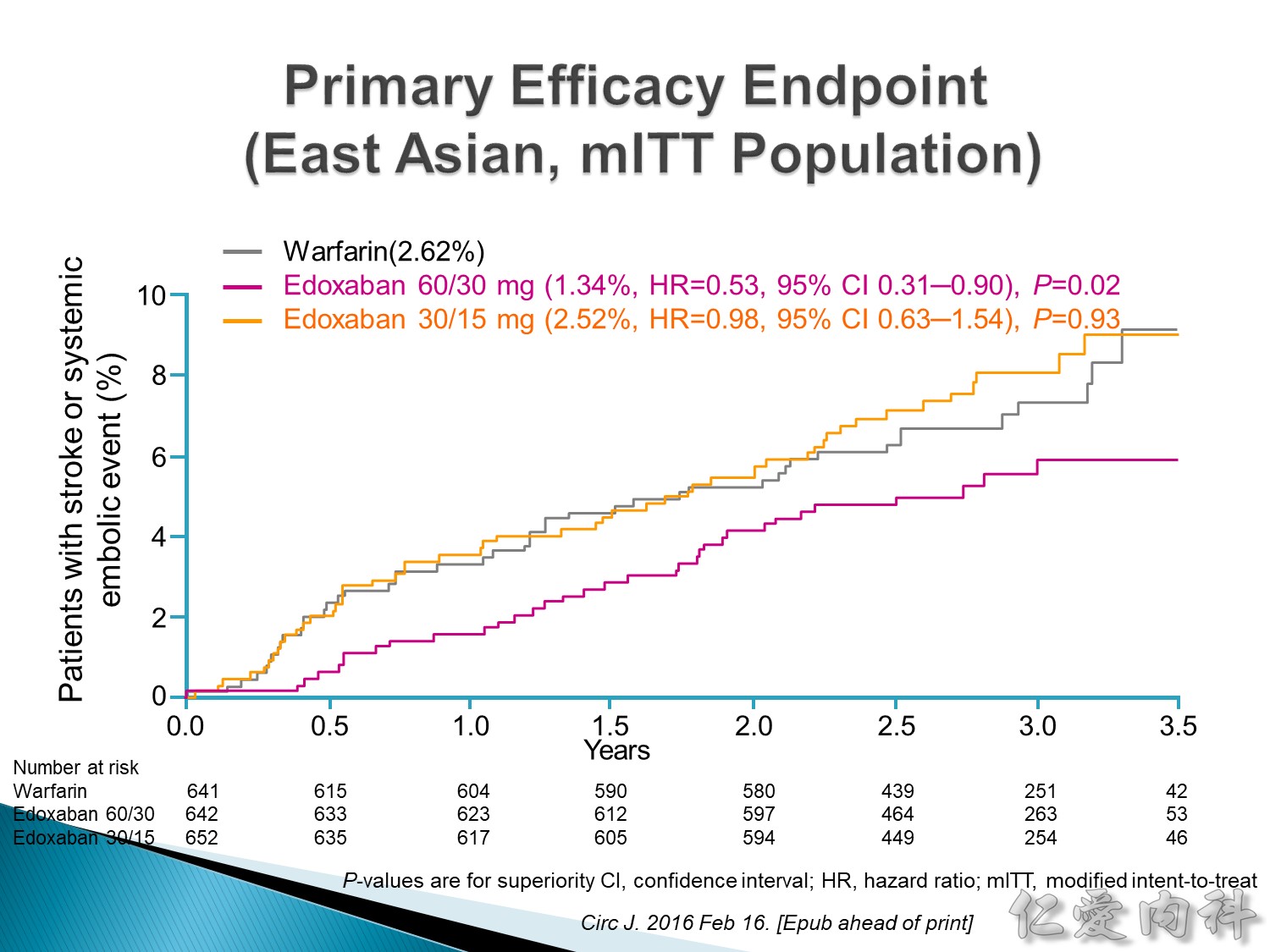
Efficacy: low-dose edoxaban 相當於 warfarin,使用標準劑量時的效果則是遠優於 warfarin 及 low-dose。
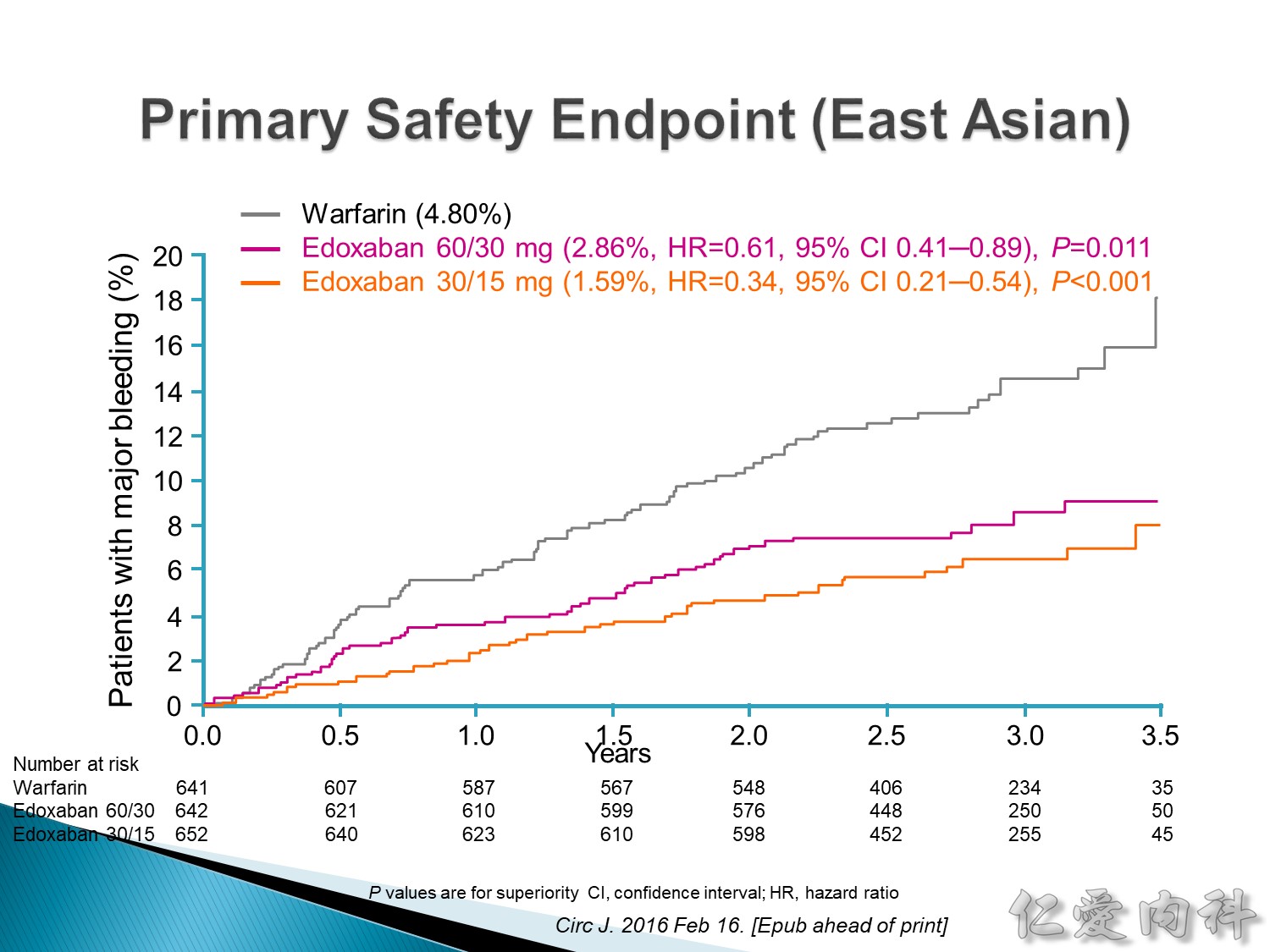 出血風險:low-dose > 標準劑量 >>>> warfarin。
出血風險:low-dose > 標準劑量 >>>> warfarin。
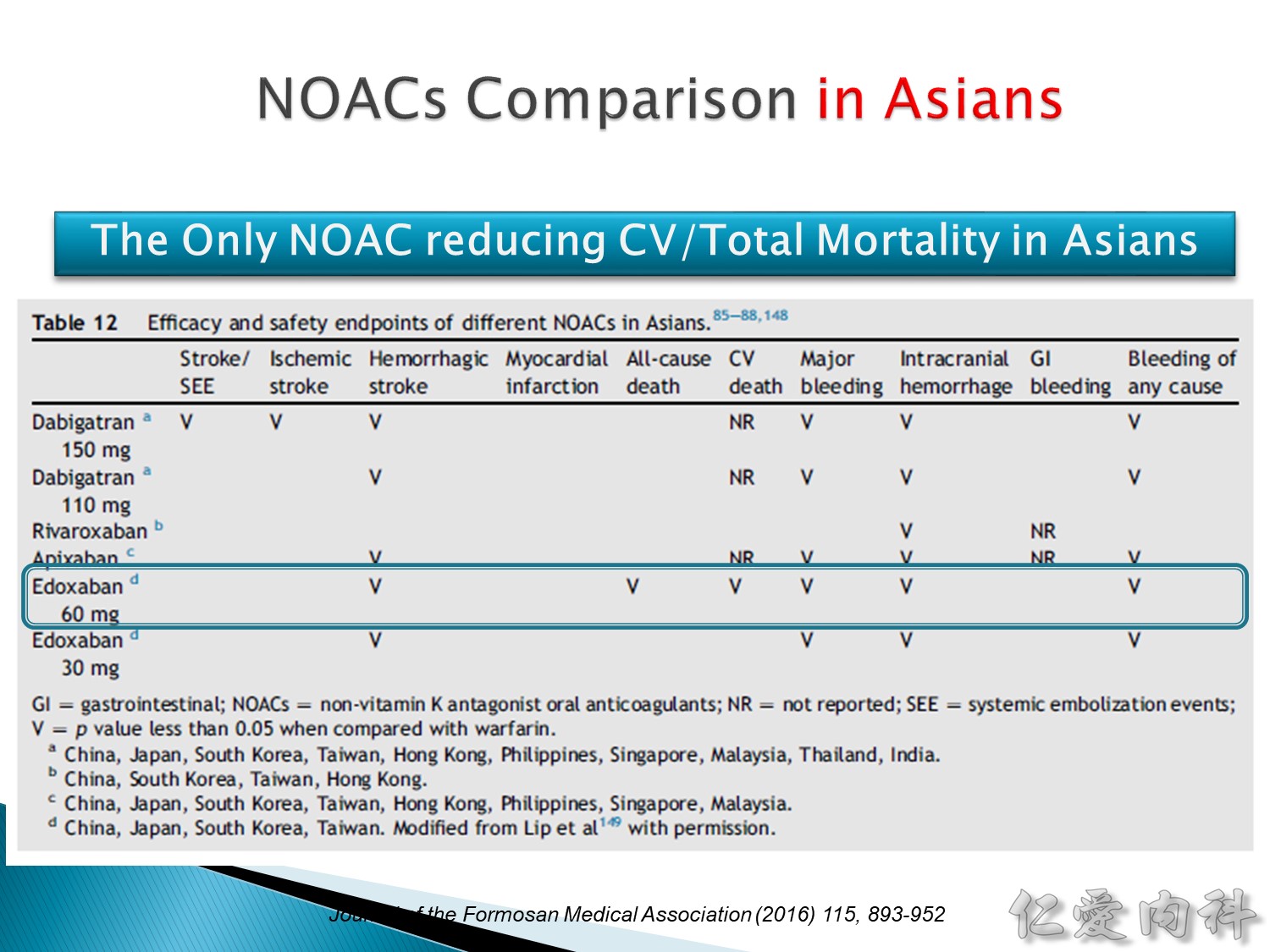
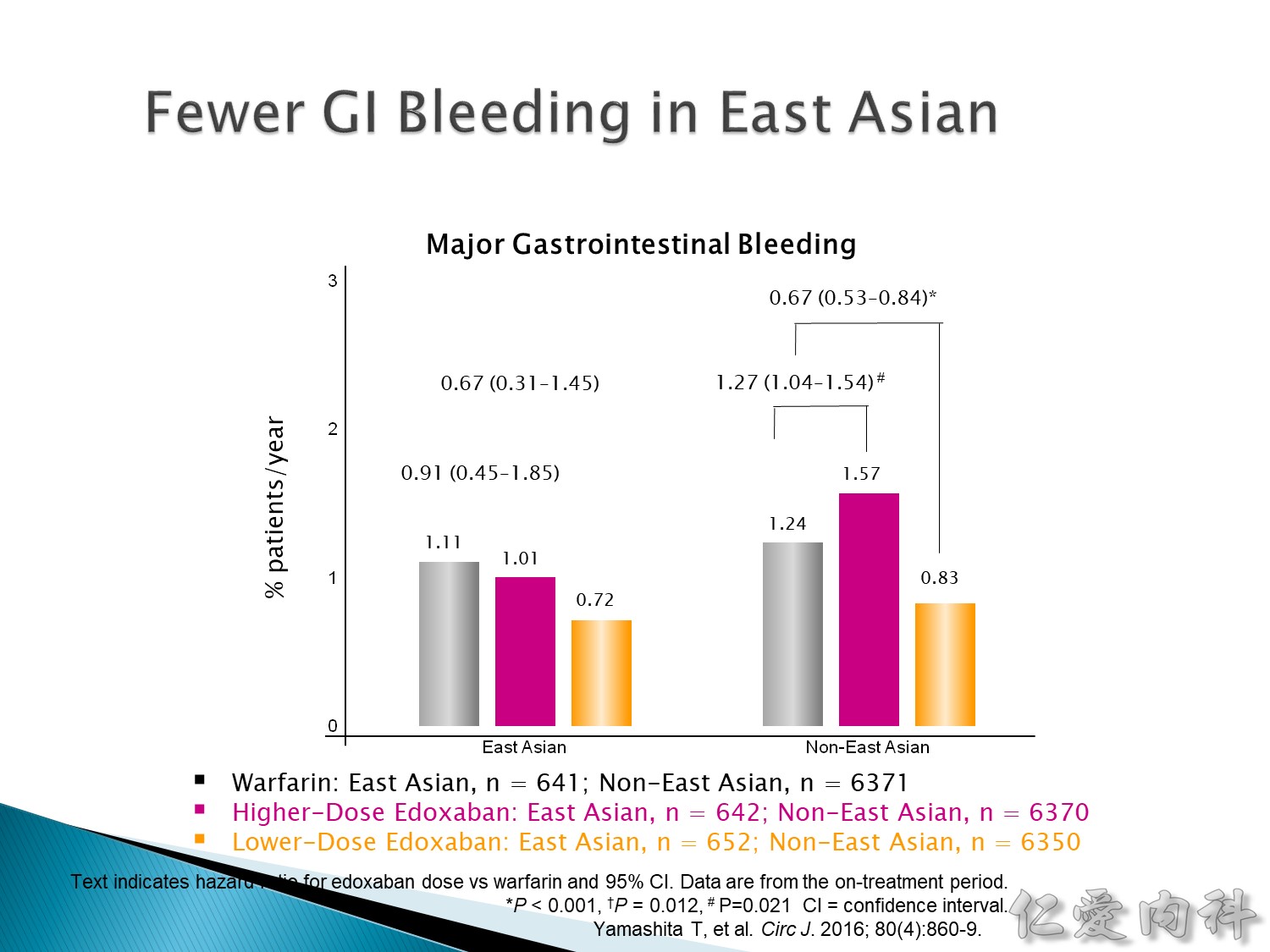
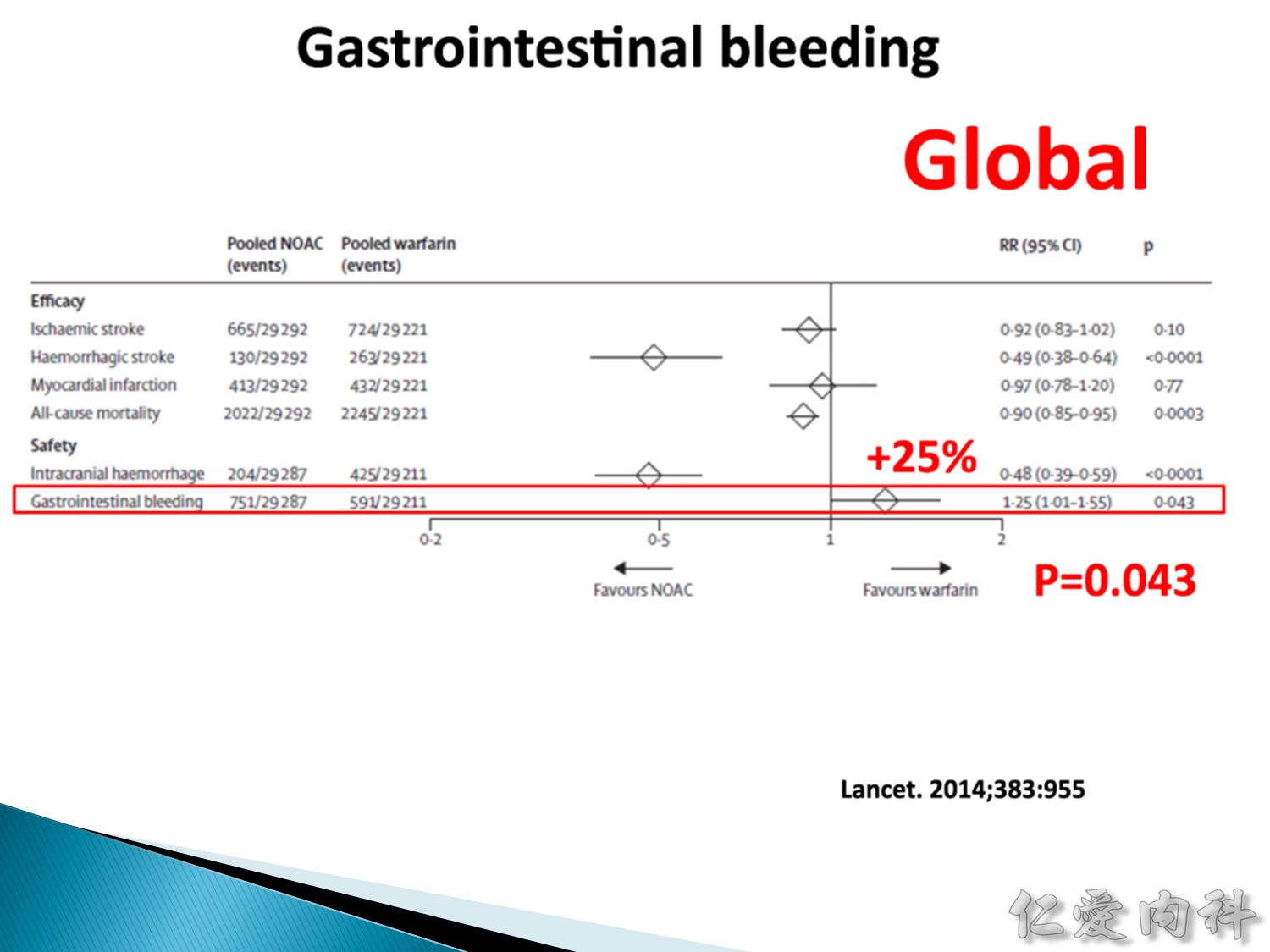
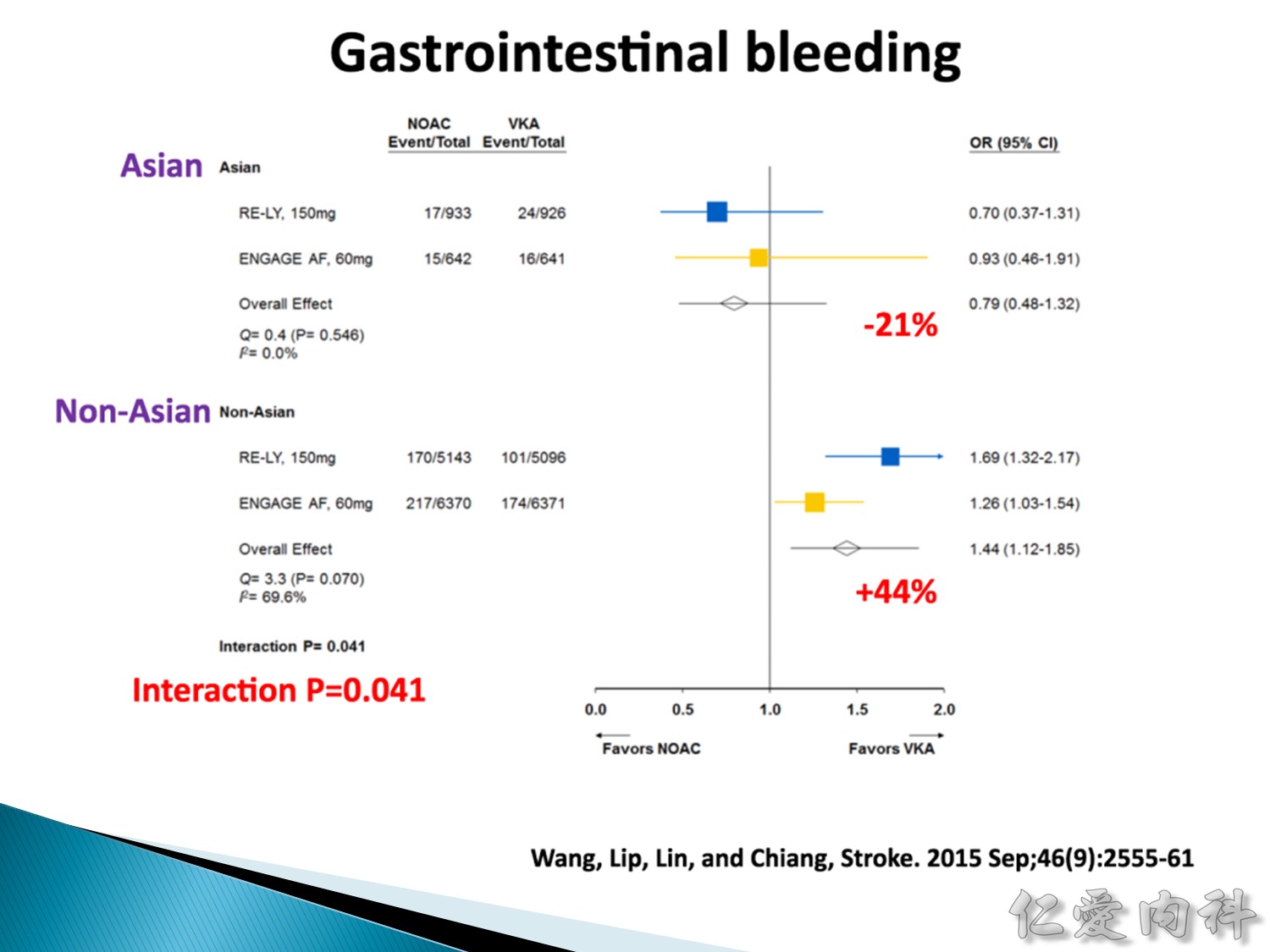
東亞族群,GI bleeding 的機率 (跟 warfarin 比較) 比較低。
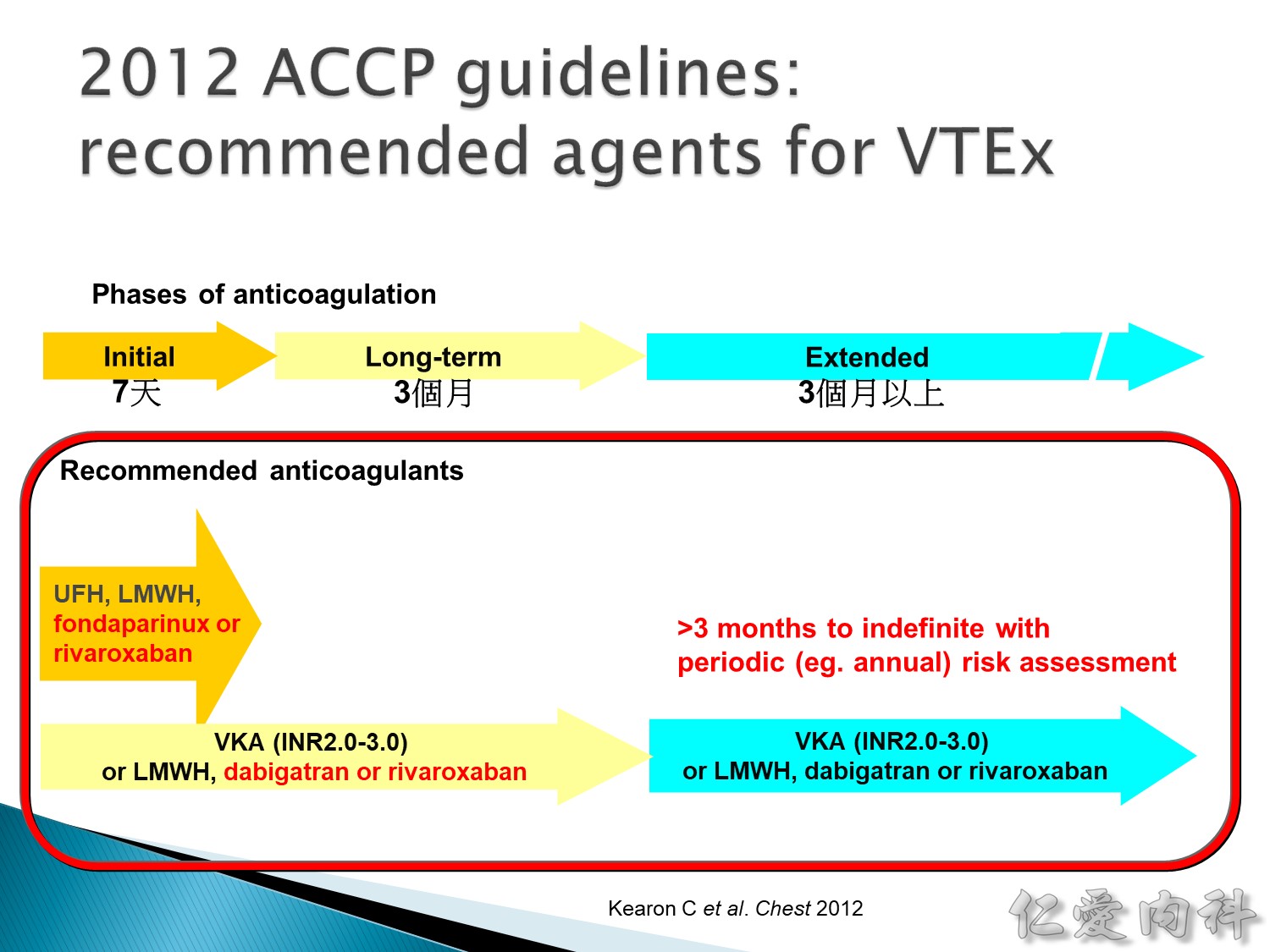
Ref: Kearon C, Akl EA, Comerota AJ, Prandoni P, Bounameaux H, Goldhaber SZ, Nelson ME, Wells PS, Gould MK, Dentali F, Crowther M, Kahn SR. Chest. 2012 Feb;141(2 Suppl):e419S-94S.
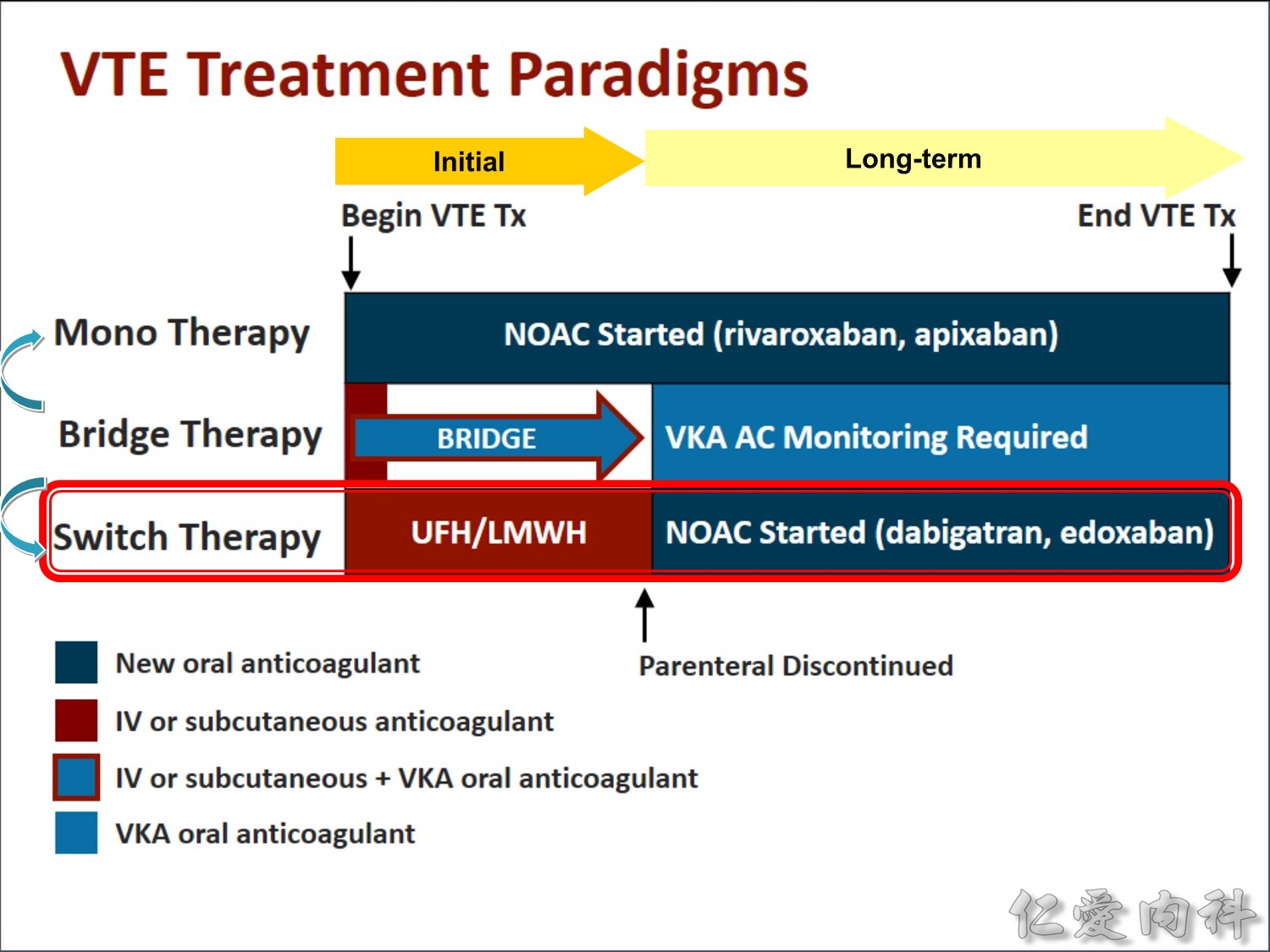
Monotherapy:一開始就使用 NOAC。
Cancer 病人的血栓發生率較高,認為打針的效果比口服 NOAC 來的要好 (NOAC的效果還在試驗中)。

Q&A
1. 解毒劑?
FDA 有 proved antidote 但沒有商業化,andexanet alfa (針對 Xa 的)。
2. 不同的 NOAC 之間轉換如何轉換?
直接換就好,因為 half-life 都 12 小時,而且 onset 很快
3. 要考慮很多議題
1) 手術、biopsy、要不要停? 停多久? 什麼時候吃回去?
2) 吃了 NOAC 預防中風但還是中風,要怎麼辦?
3) 如果在吃 DAPT 或是有塗藥支架,NOAC 要不要繼續吃? 怎麼吃?
您也可以參考: 口服抗凝血劑與中風之案例分享 – NOAC in Stroke 2018 Case Sharing。