作者/講者: 張哲誠 醫師
整理/校稿: 劉舜傑 醫師
上次校閱: 2018/08

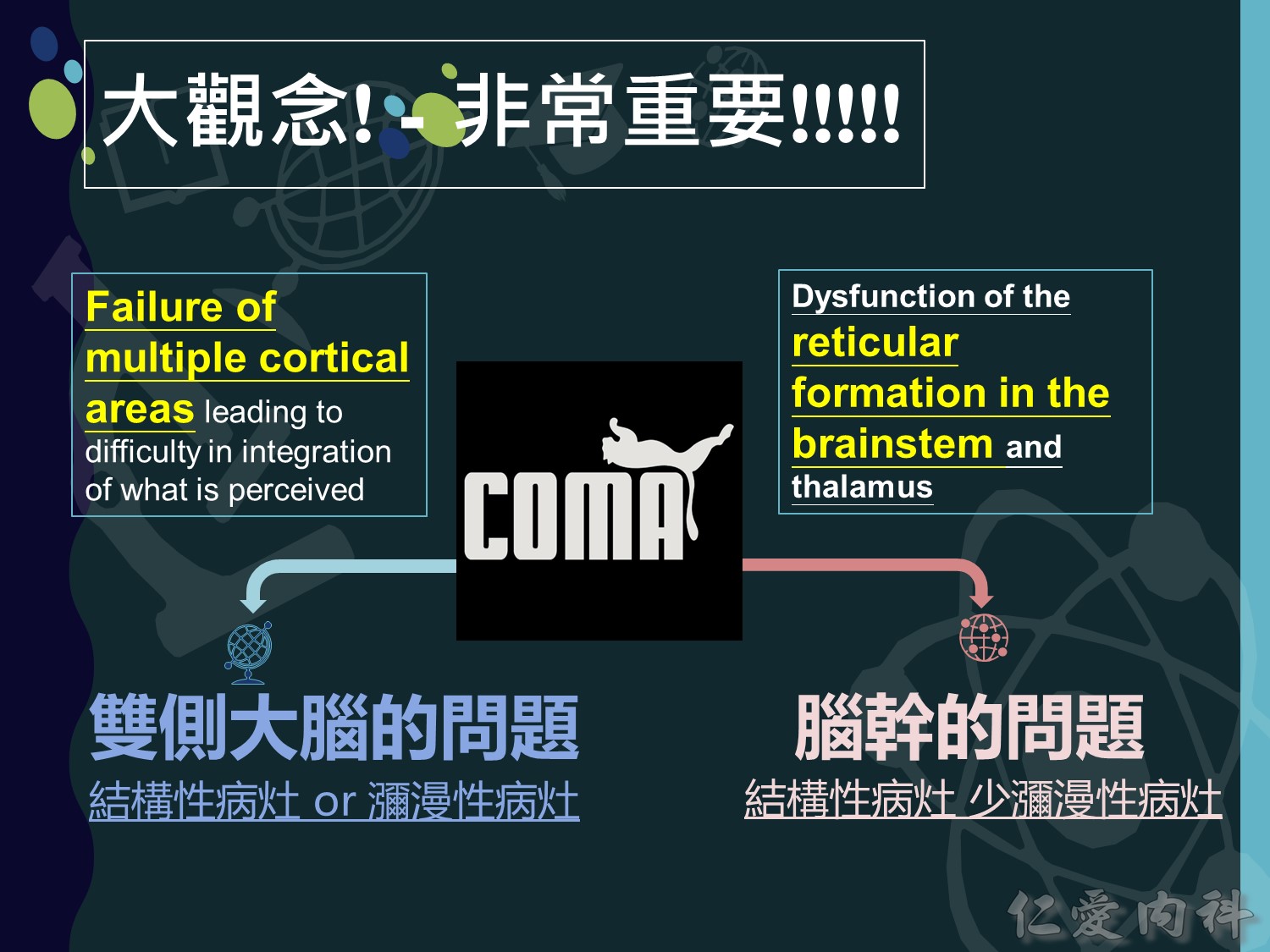
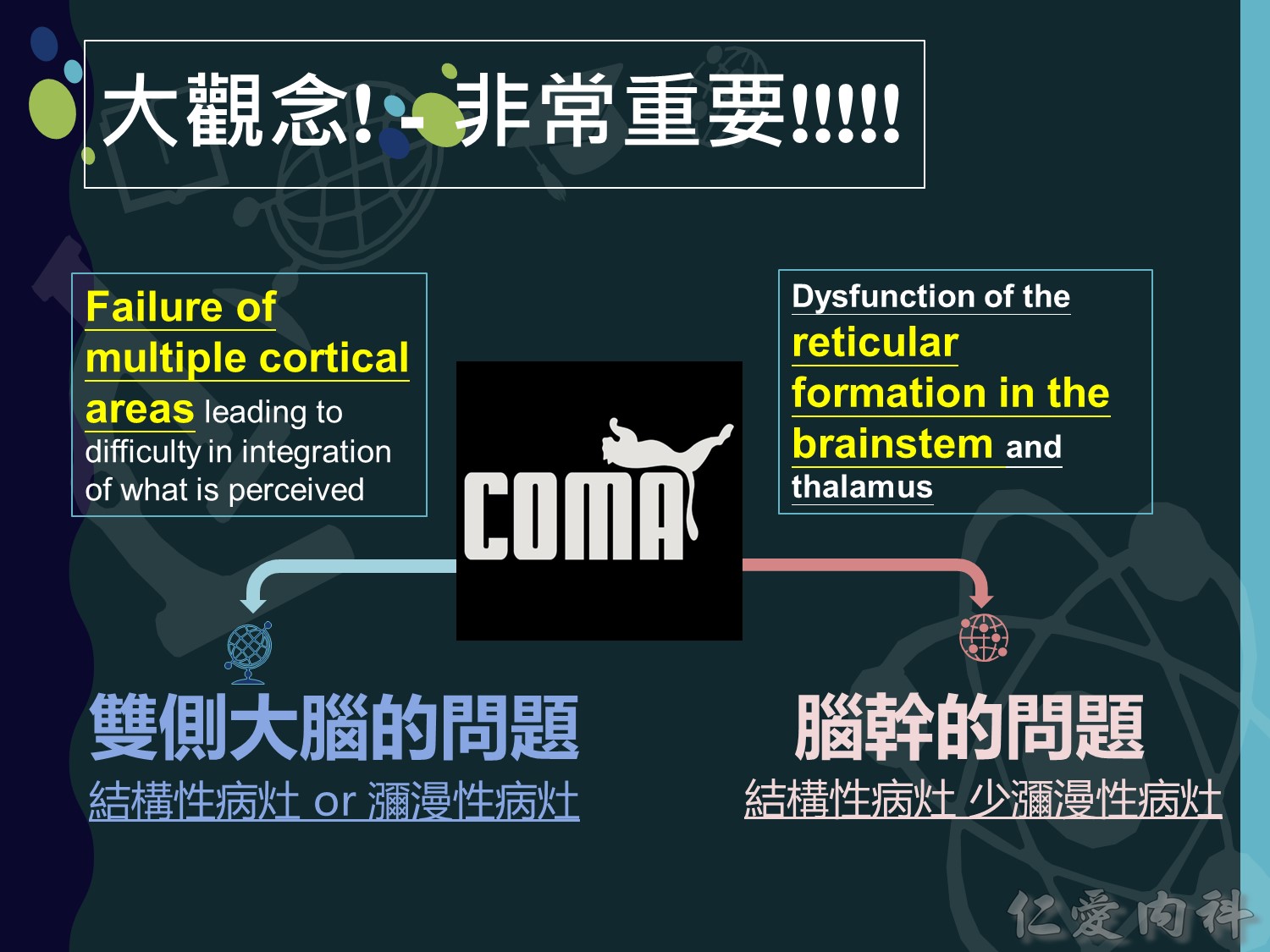
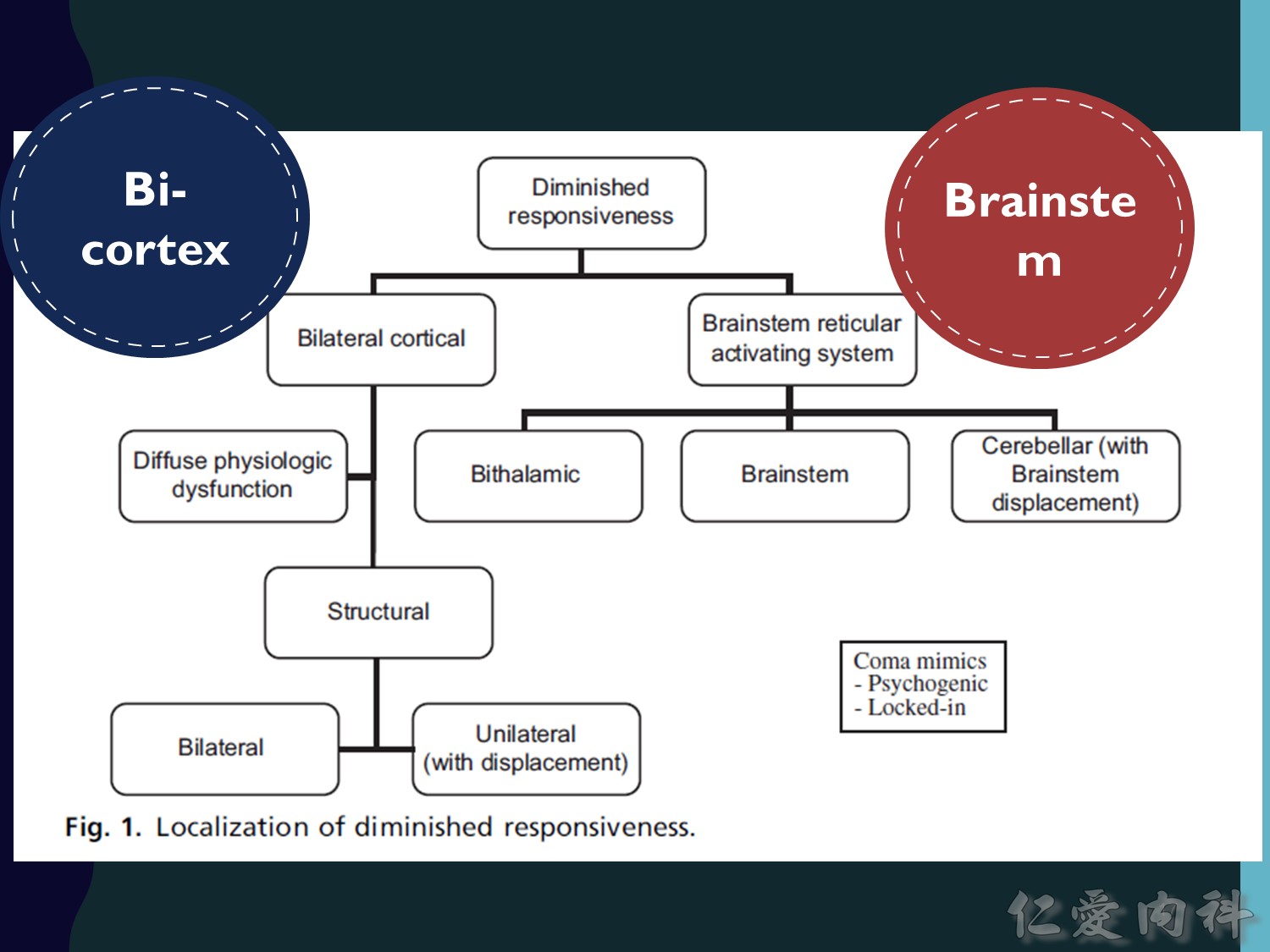
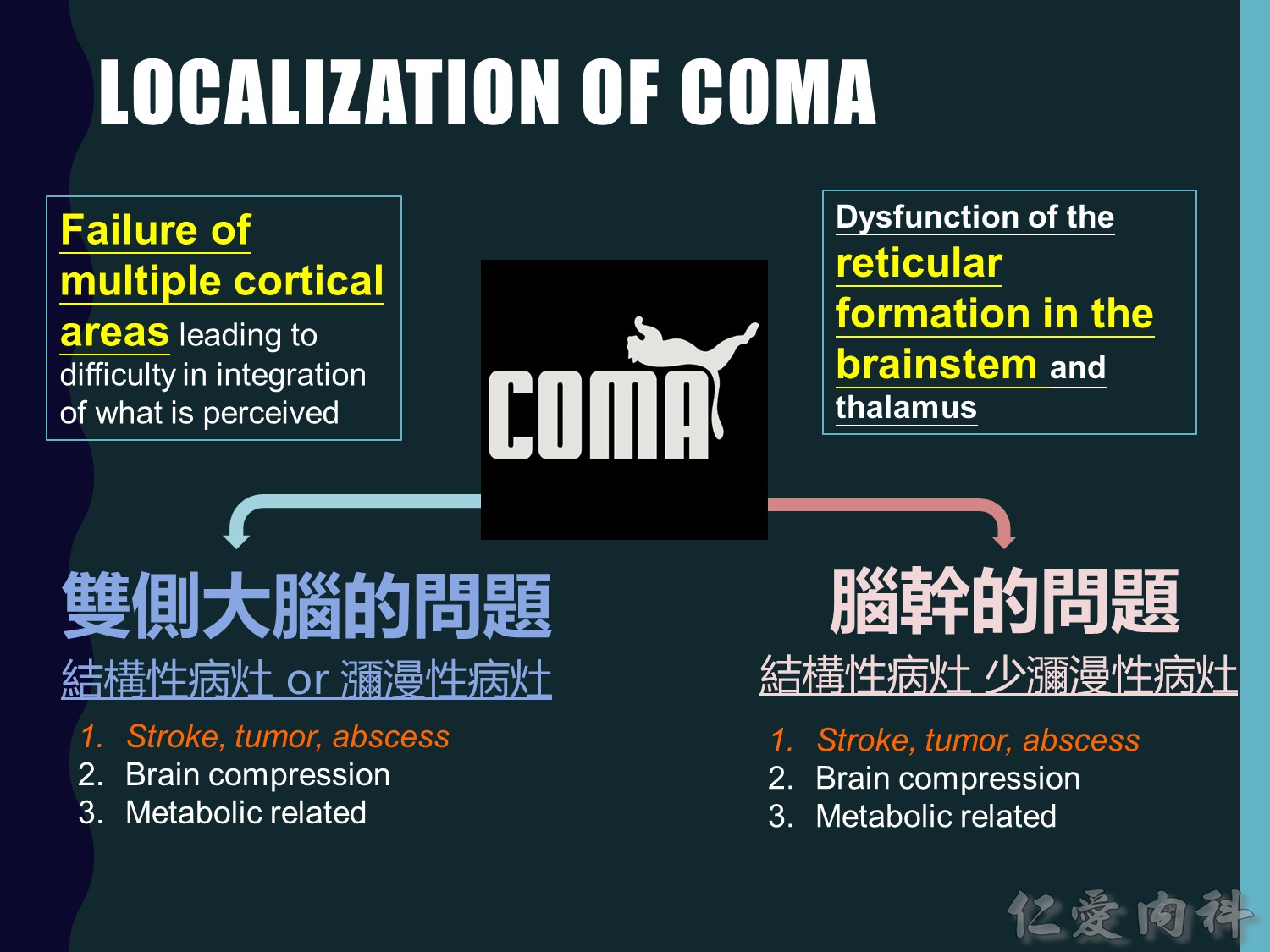
如果只想看一張圖 這張是最重要的 整個主題的核心
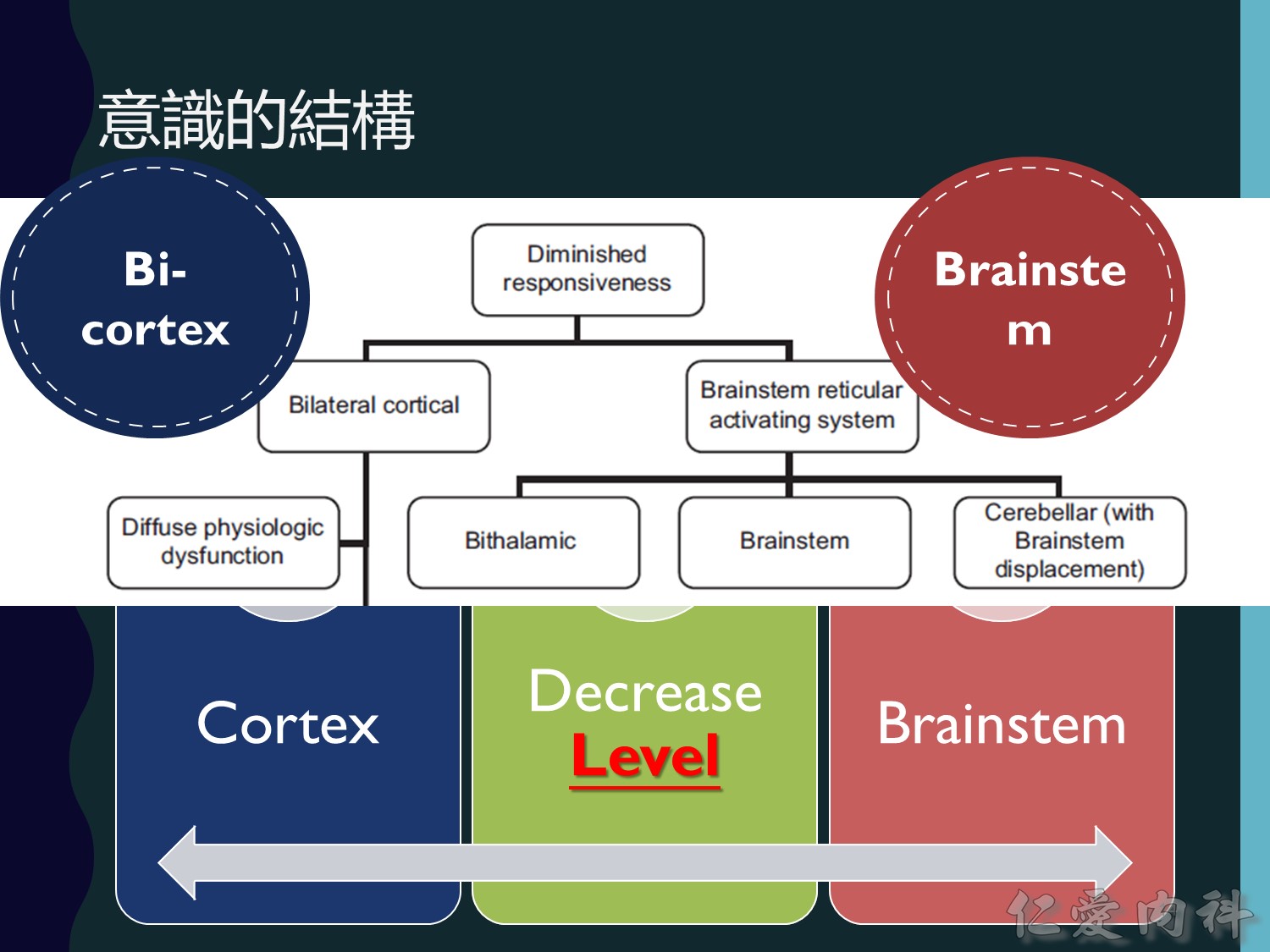
COMA 兩大原因:
- “雙側”大腦 或
- 腦幹
Harrion 加了第三個原因:
- Supression of reticulocerebral function by drug, toxins, or metabolic derangements
加Harrison 的 approach:
會死人的respiratory / cardiovascular acute problem 先處理 在評估coma的原因跟嚴重度
History
1.什麼情況下發生 進展速度
2.Antecedent symptoms (confusion, N/V, fever, seizure, dizziness..)
3.Drug/Toxin/alcohol?
4.任何慢性肝腎心肺問題?
PE:
Fever 很少是central fever (hypothalamic lesion), Seizure 會稍微上升溫度 ,酒精藥物低血糖會低體溫 ,低體溫本身也會coma
BP 高要想到 hypertensive encephalopathy ,腦出血,Trauma
BP 低要想到 sedative 及 其他Shock的Ddx ( MI , hypothyroidism/ adrenal crisis,/ sepsis/ hemorrhagic shock)
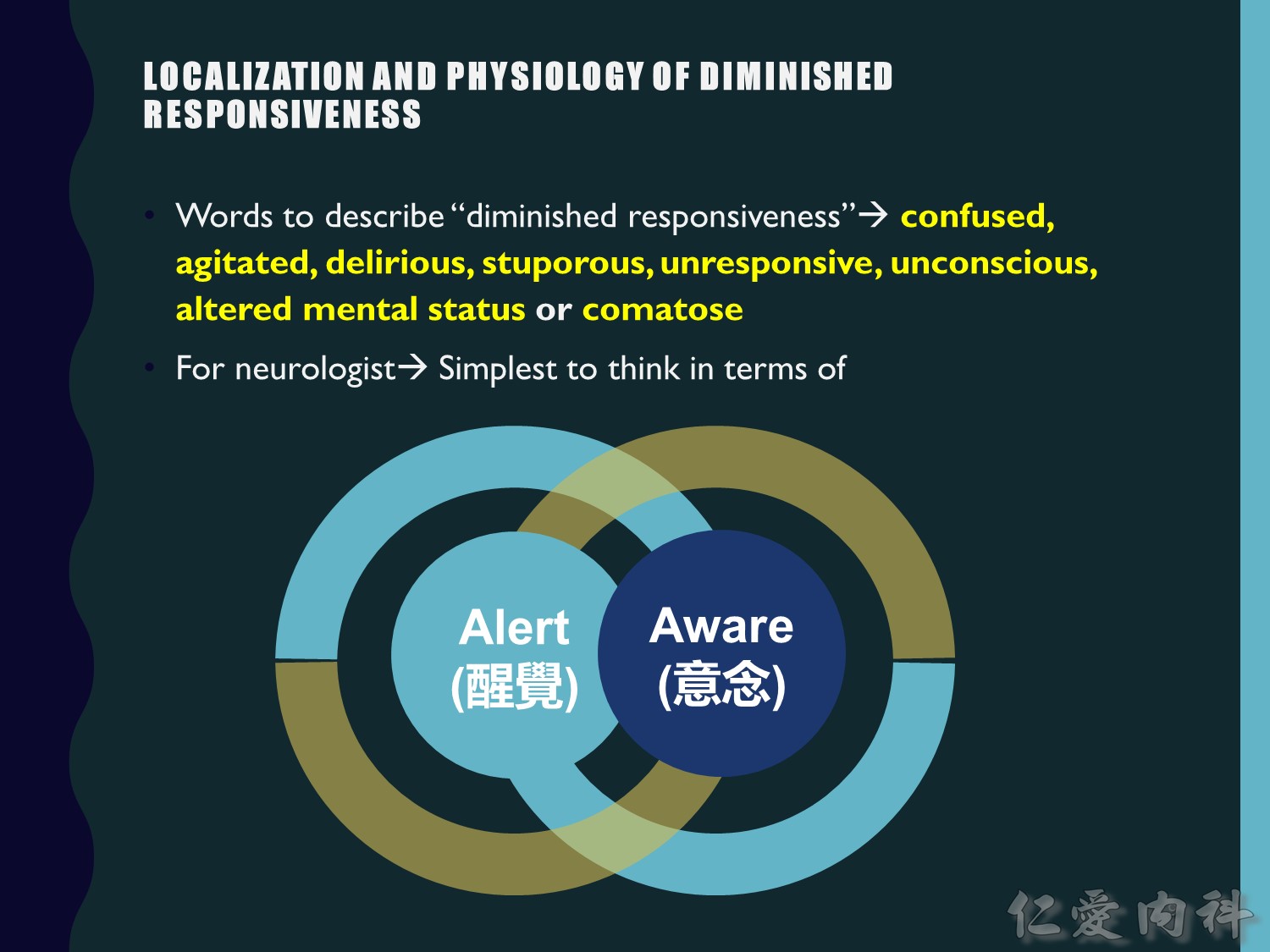
我找到的impaired consciousness的定義 ,
1.A disturbance of arousal leads to diminished alertness– RAS 問題
2.A disturbance involving content leads to diminished awareness- multiple cortical function問題
這兩者可同時存在 同時不存在 或只有存在一個
為了簡化臨床問題 只討論 Alertness
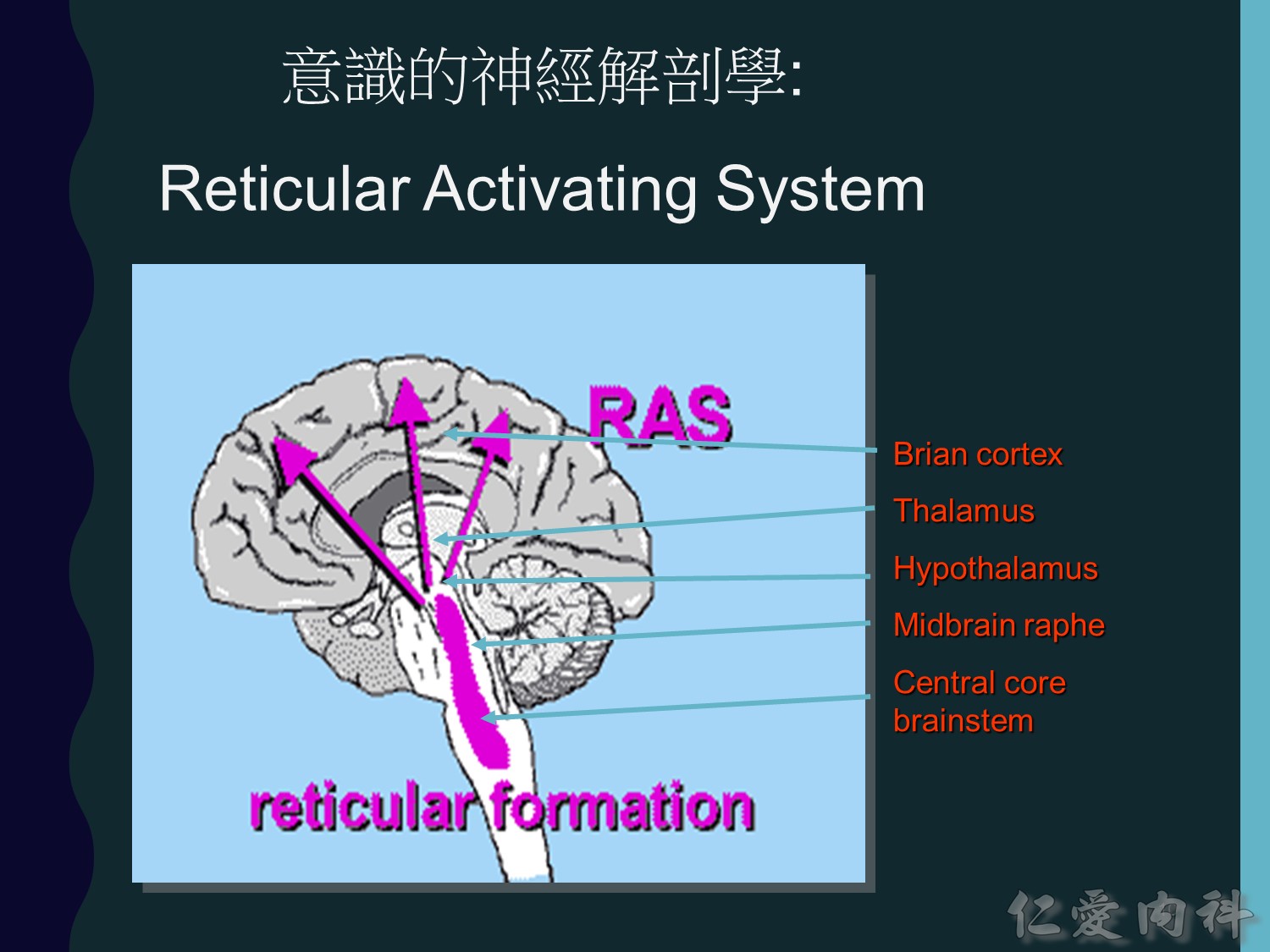
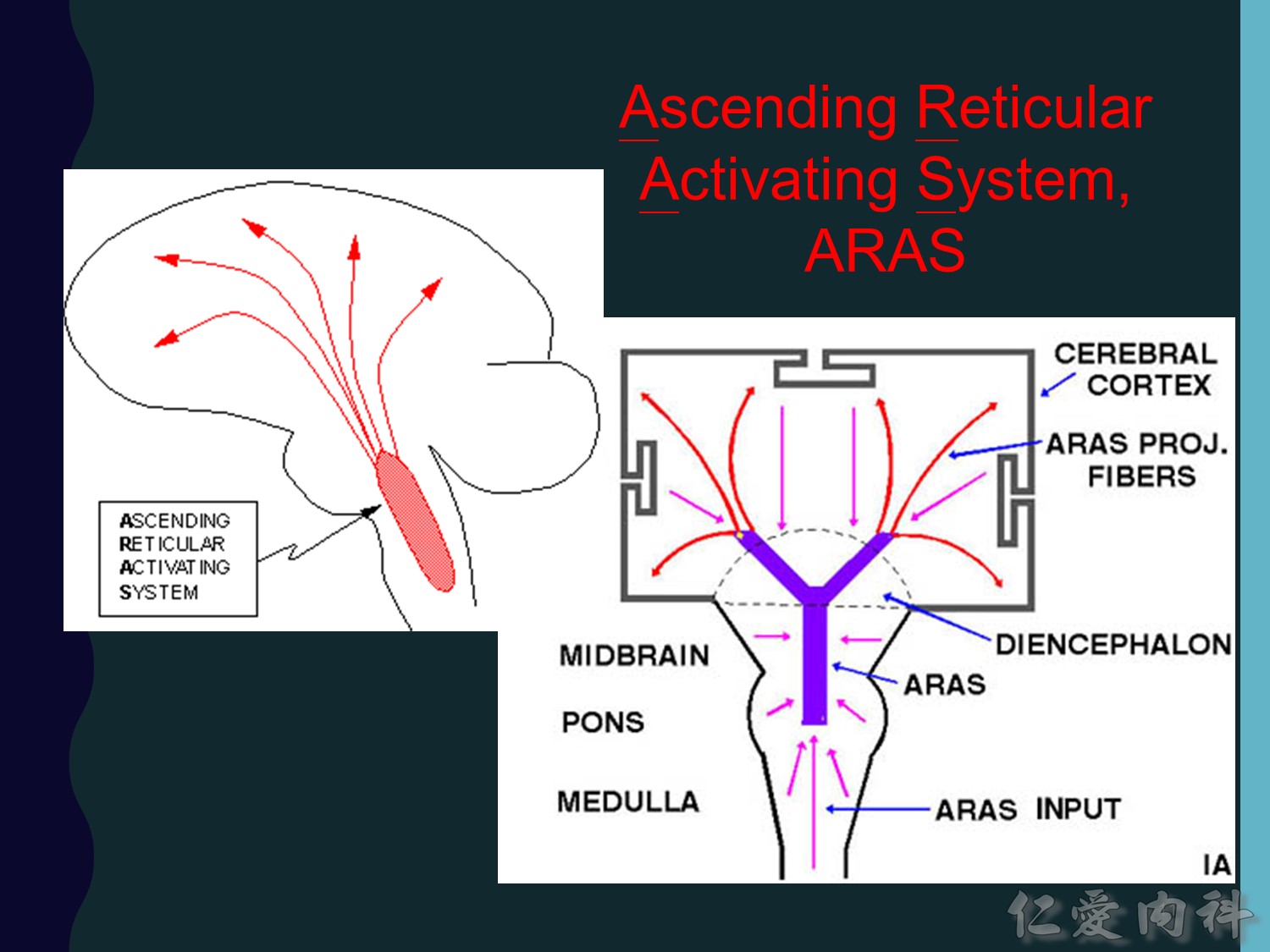
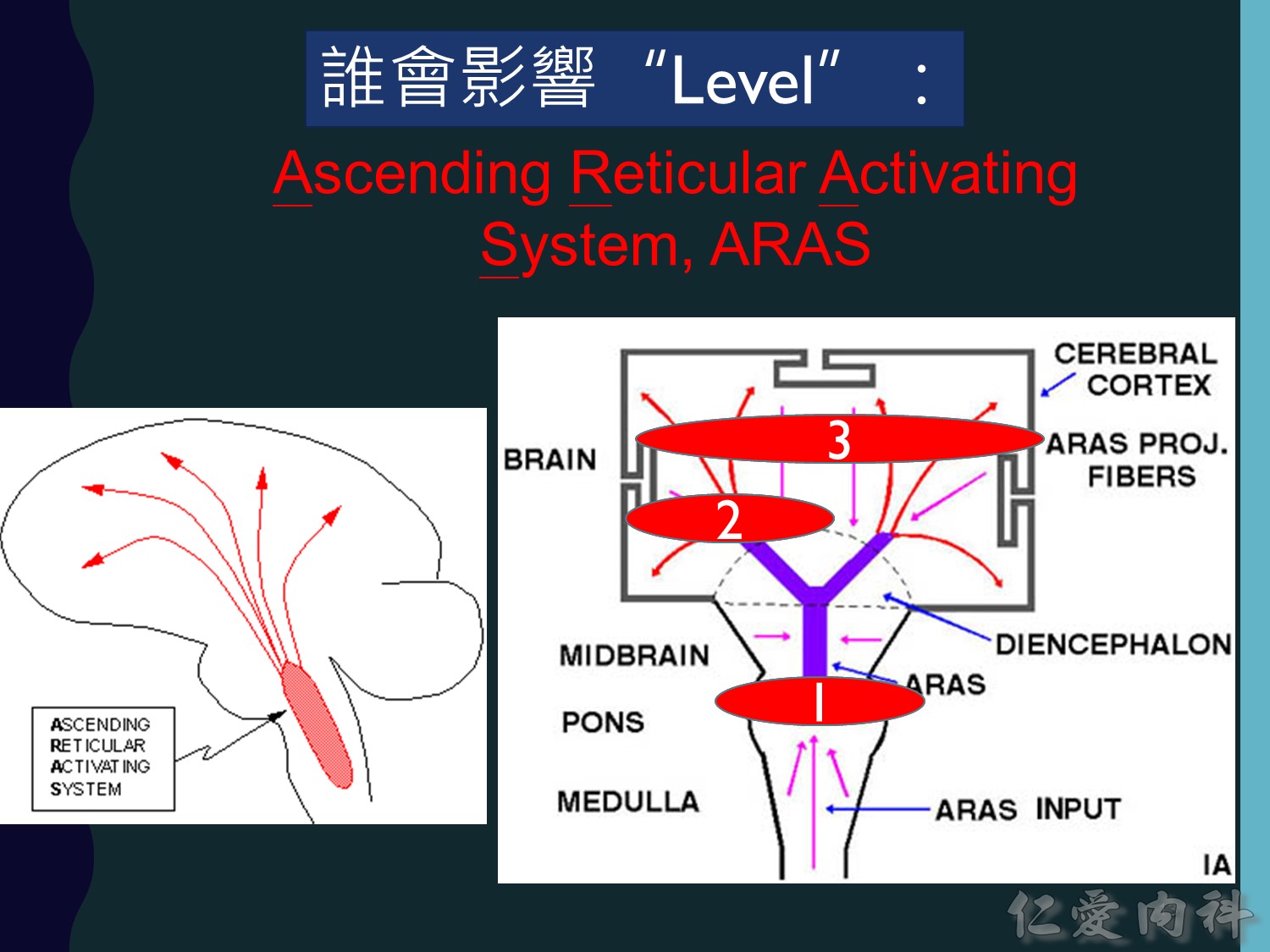
如圖 要產生Coma 必須要有 ascending RAS 到雙側大腦的路徑受到損傷
所以Thalamus其實是很重要 維持arousal的地方
但為了方便記憶大觀念,coma 或是impaired consciousness就要想到兩個問題
- 雙側大腦
- 腦幹
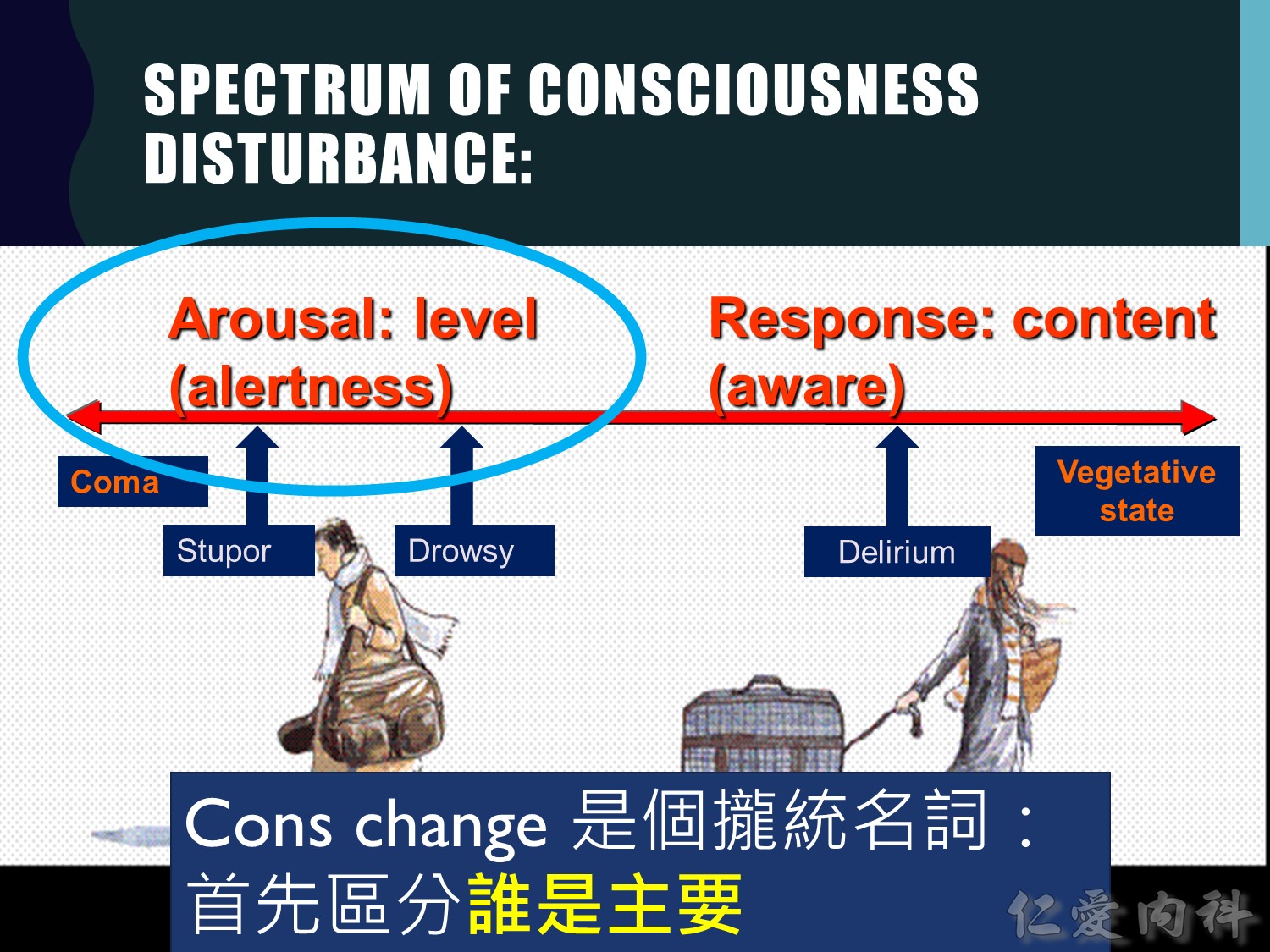
Arousal – alertness- level
Response – aware – content

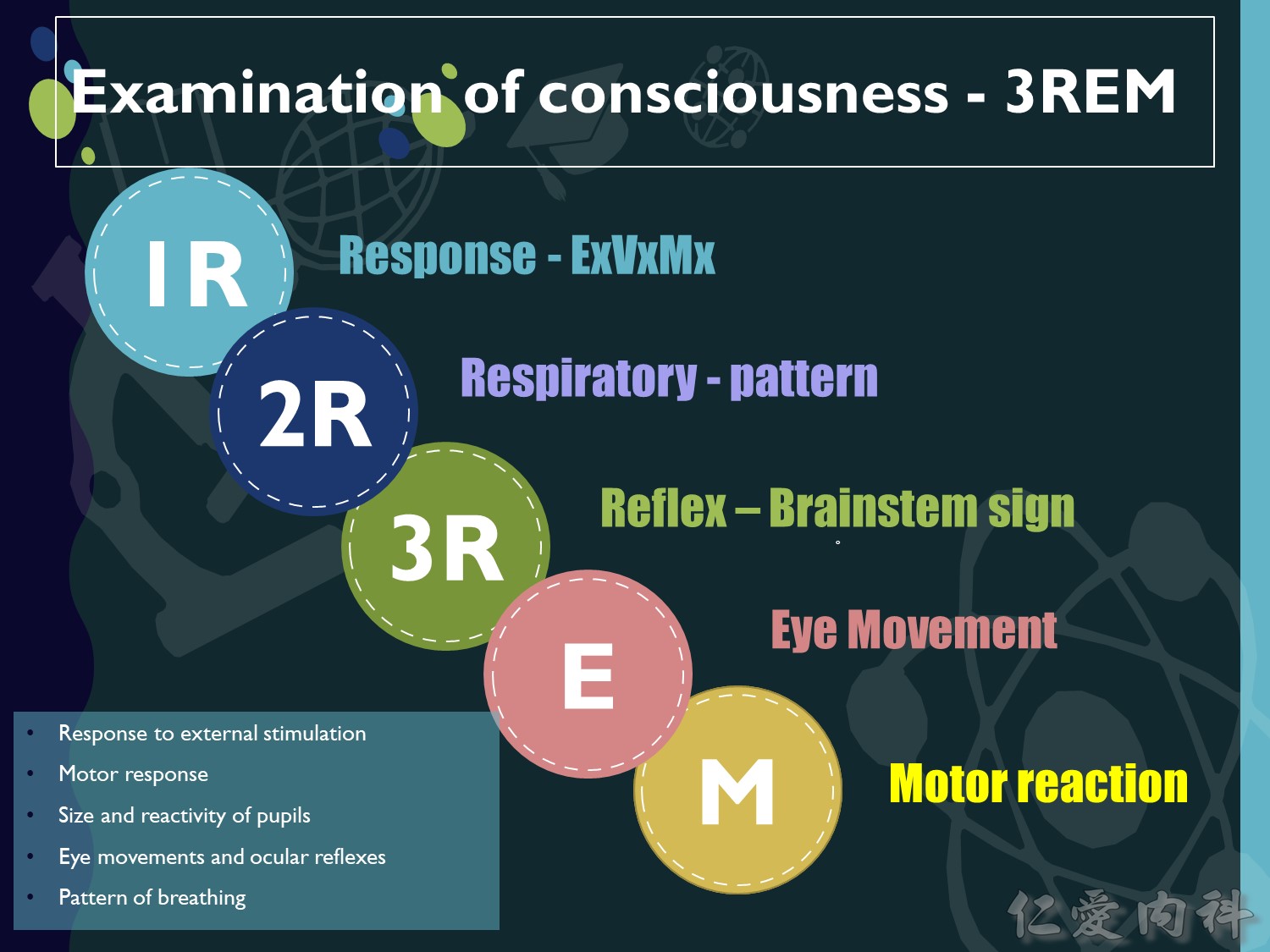
下次遇到Conscious change就是用這個口訣 3REM 去綜合評估
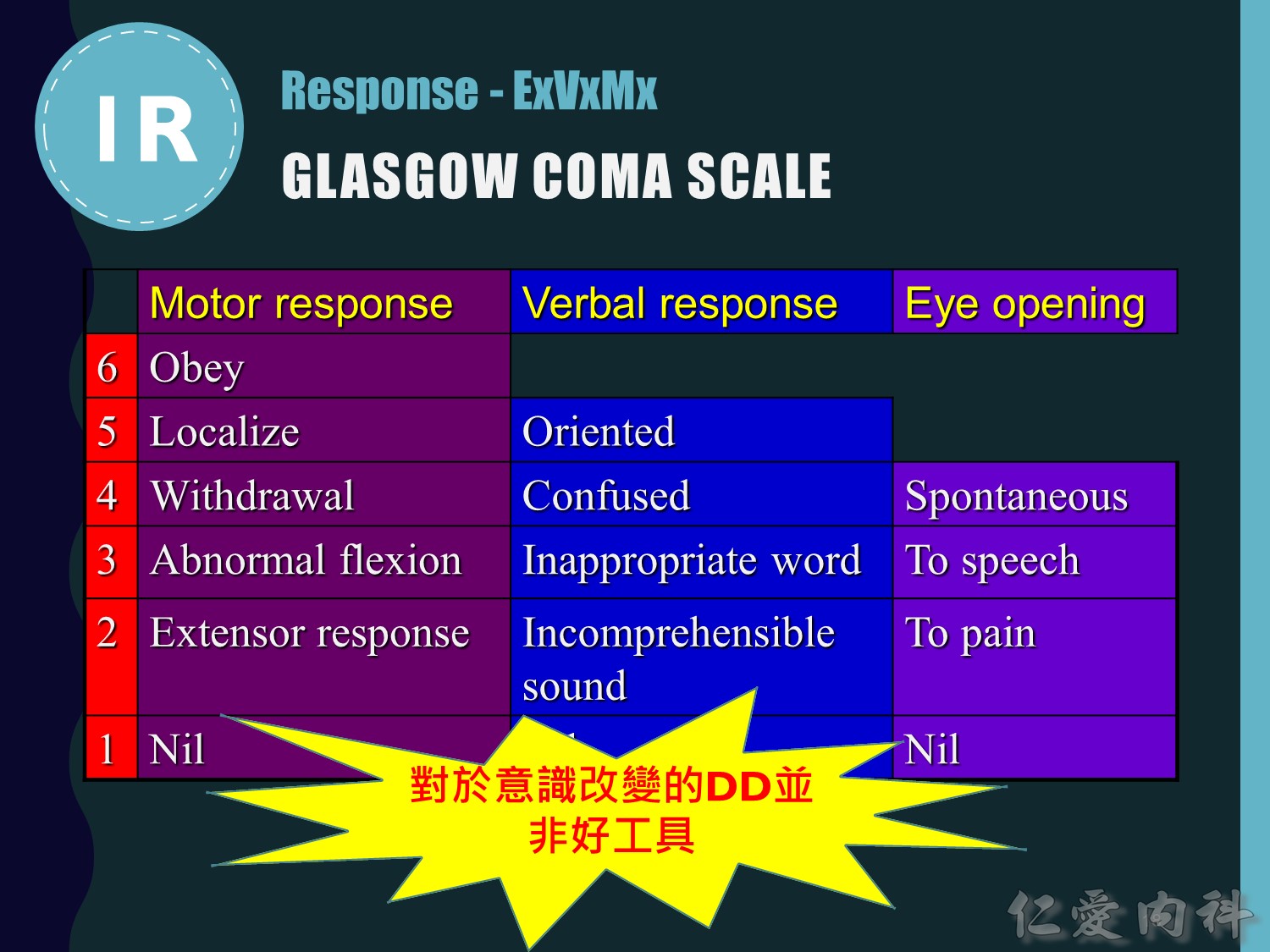
GCS是當初(1974年) neurosurgeon評估Conscious level的工具
也用了很模糊的名詞來形容 e.g. stupor, semicoma, deep coma
但很不好用 除非 分數差太多 比如14 分掉到5分 要不然針對臨床常見狀況真的很難使用
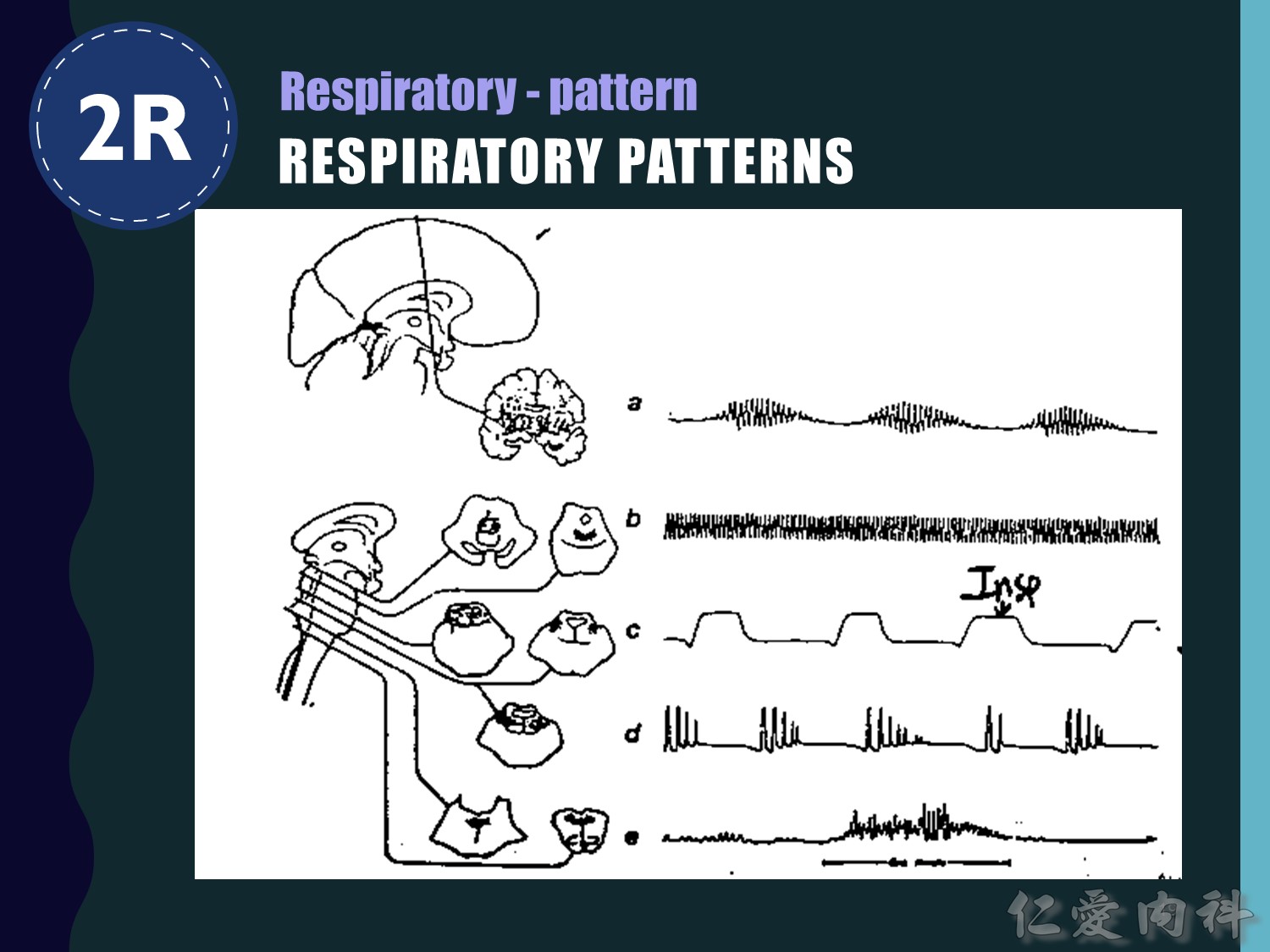
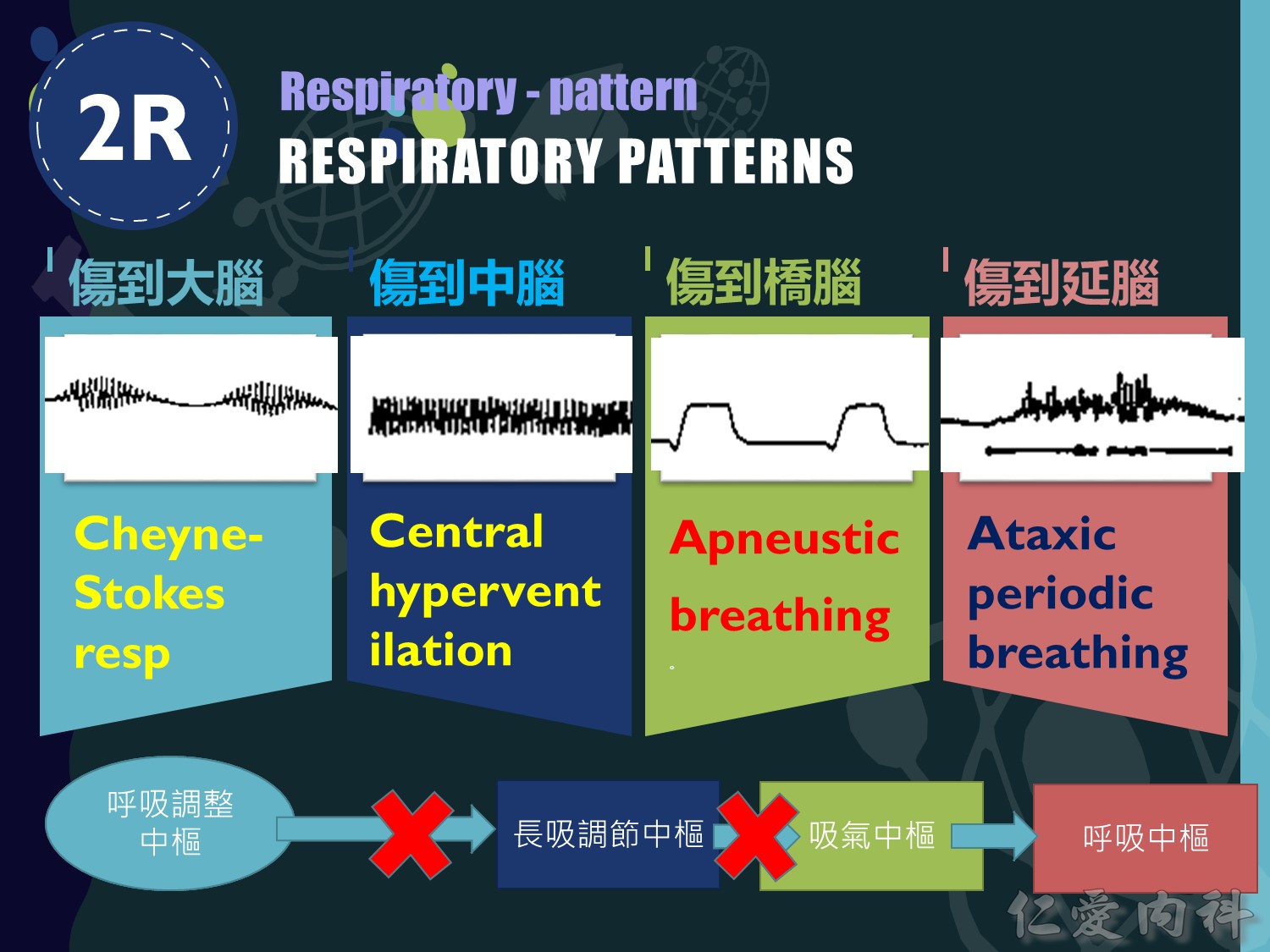
呼吸調節中樞(pneumotaxic center) -呼吸快慢深淺作精細的微調 ,可抑制長吸調節中樞
- 傷到大腦 (最常見) – Cheyne Stokes (另可見於 CPR後 , hypoxia, metabolic encephalopathy)
- 傷到中腦 –呼吸調節中樞 無法抑制 長吸調節中樞 ==> 長吸調節中樞 就不斷抑制 吸氣中樞 ==> 吸了馬上就吐 ==> central hyperventilation (另可見於 hepatic coma)
- 傷到橋腦-長吸調節中樞 無法抑制 吸氣中樞 ==> 一直吸,但CO2高了還是得吐 ==> apneustic breathing (另可見於hypoglycemia )
- 傷到延腦 (也常見) – 就是亂吸 忽快忽慢 (另可見於 sedative)
跟 COPD pneumonia 做鑑別診斷 ==> ABG
或許一開始喘的gas pattern不一定 ,最終呼吸衰竭的產物都是CO2 retention
但腦傷最後都是 CO2 washout
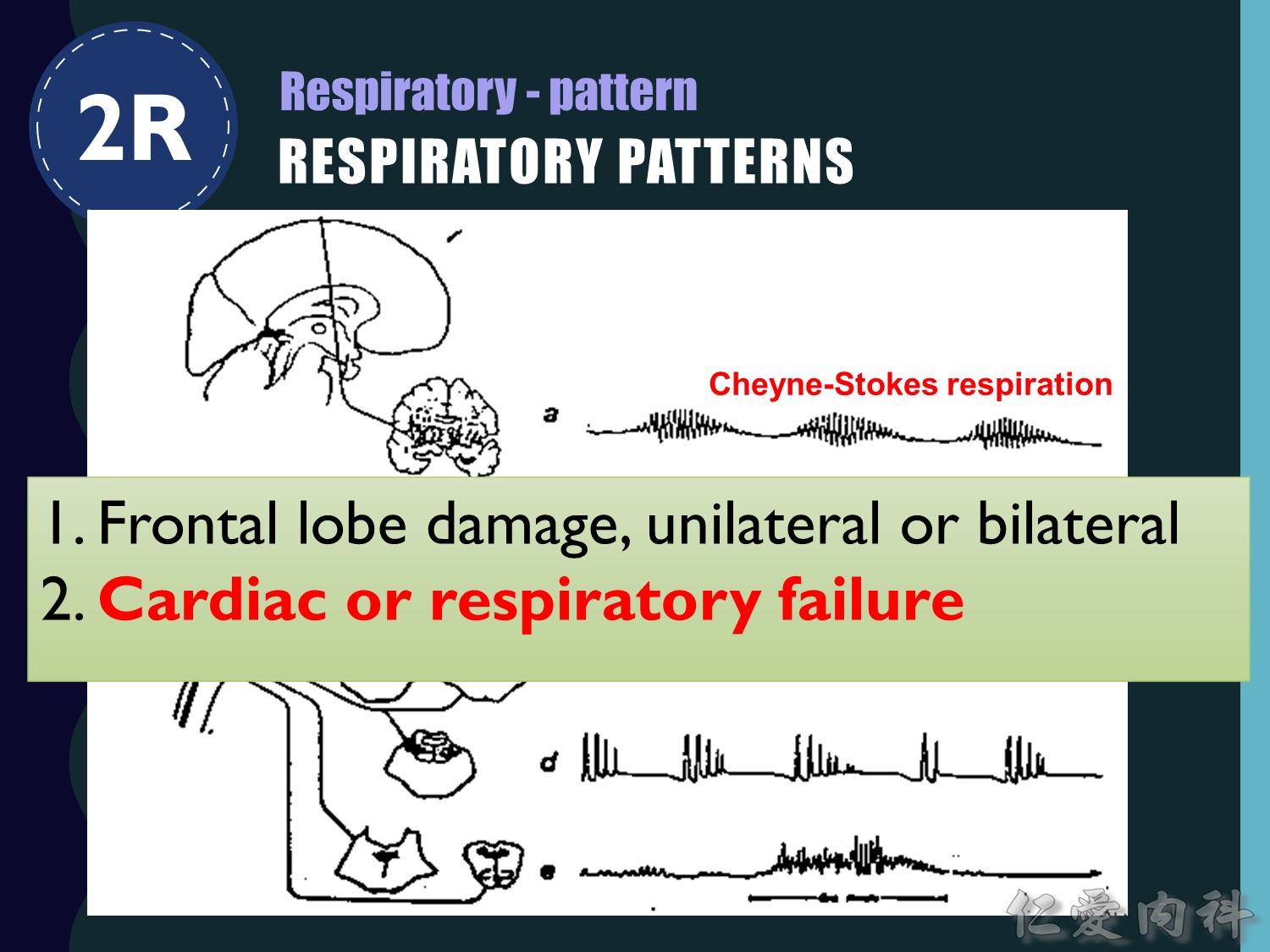
Periodic breathing, crescendo-decrescendo
The result of the loss of frontal lobe controls
Blood PCO2 drives brain stem respiratory center
Post-hyperventilation apnea
Causes
Frontal lobe damage, unilateral or bilateral
Secondary to cardiac or respiratory failure
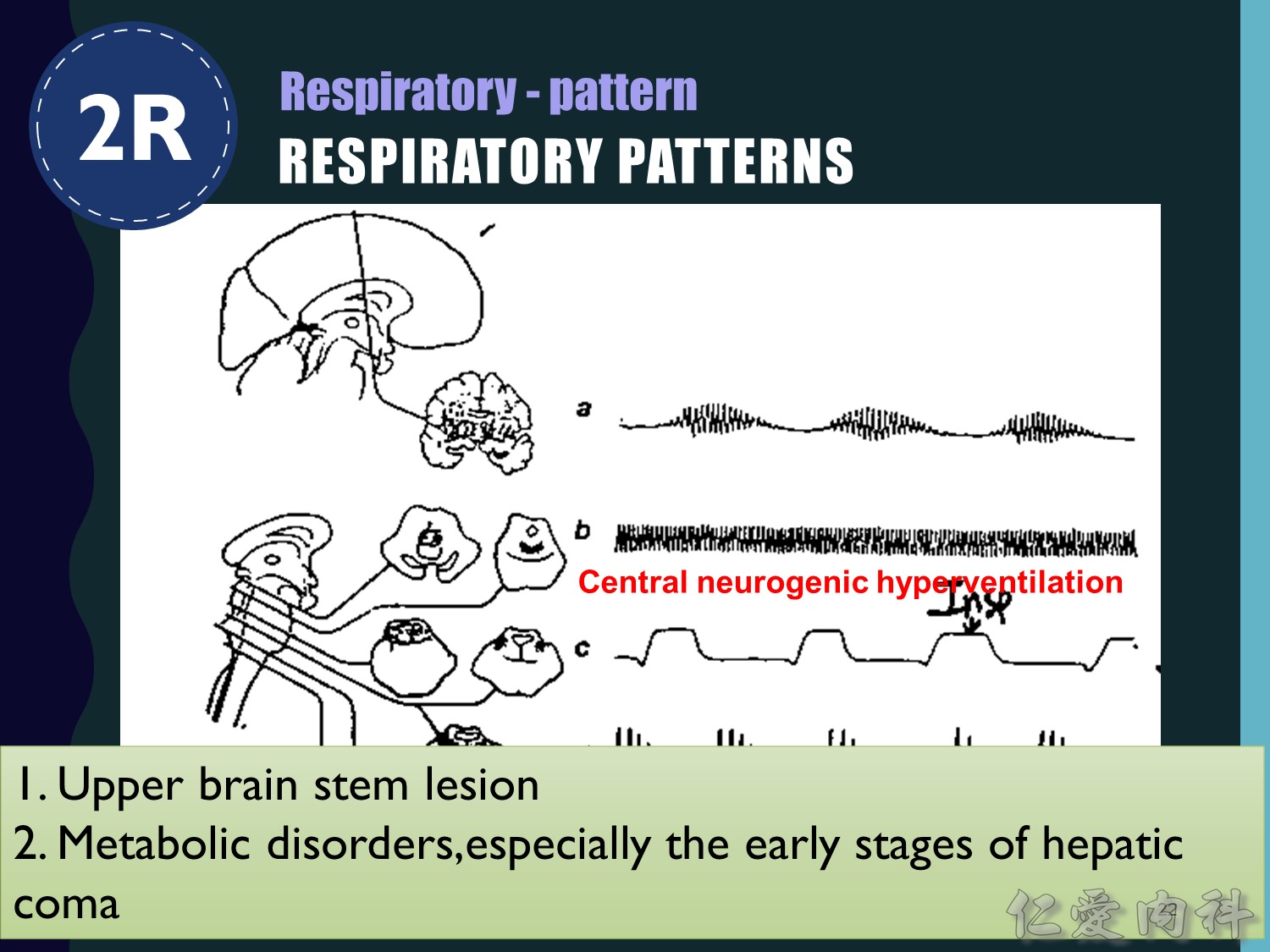
Sustained, rapid, deep hyperpnea
Not secondary to hypoxemia and acidemia
Causes
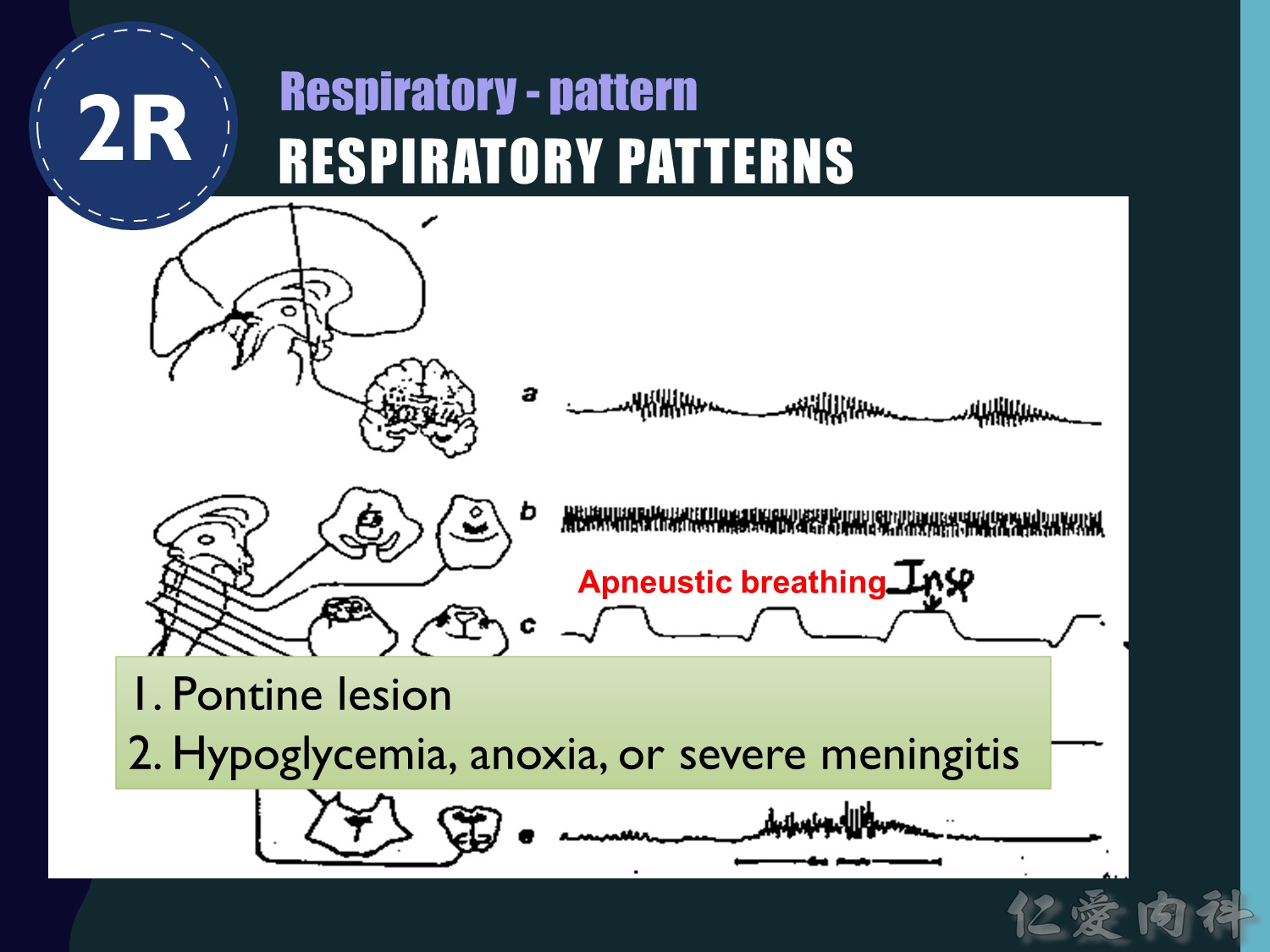
Prolonged inspiratory gasp
Discrete lesions of the mid-to-lower pons
Need early intubation and ventilation
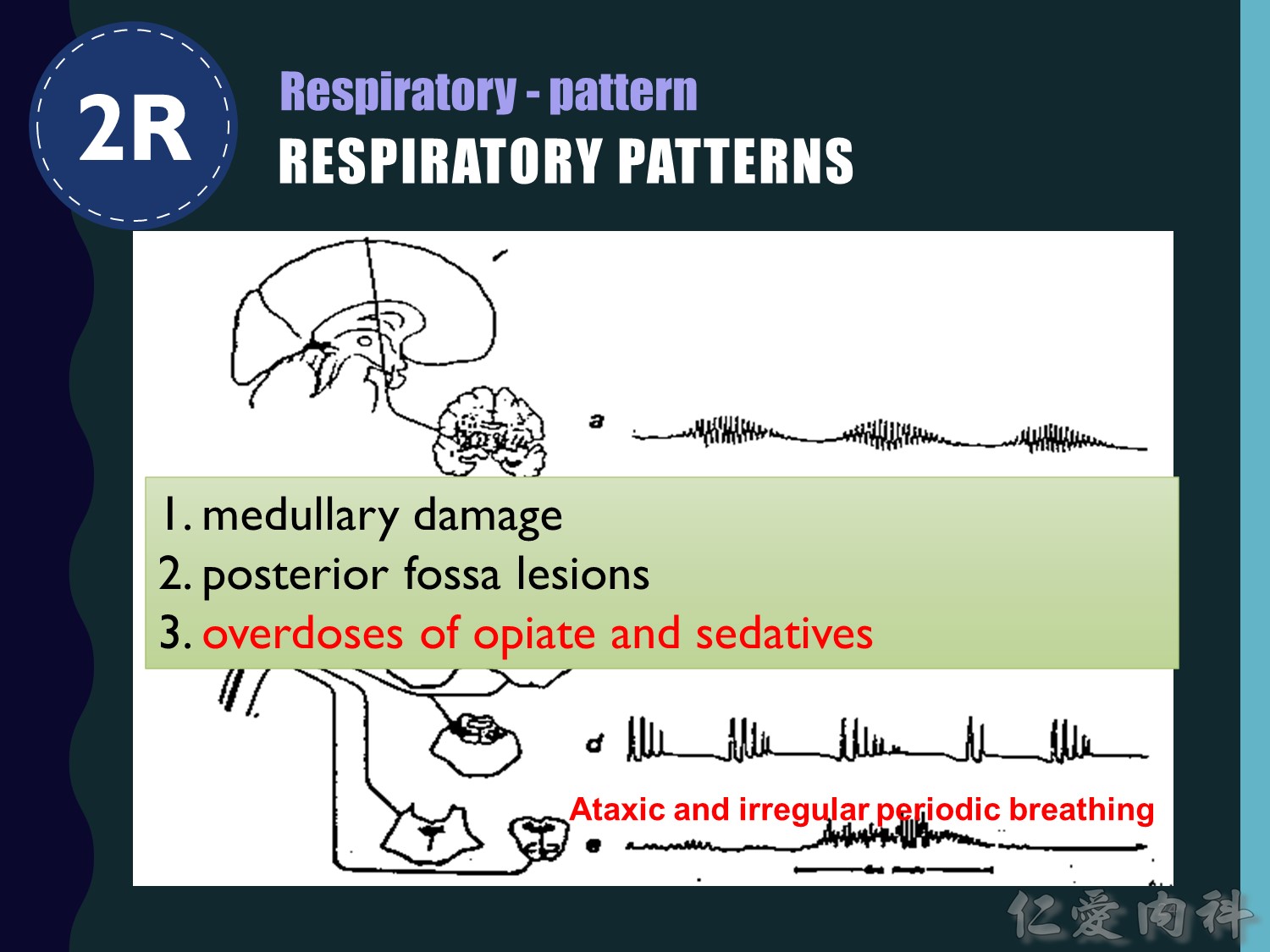
Completely irregular pattern
Slow and progressed to apnea
Respiratory center – dorsomedial medulla
Terminal states
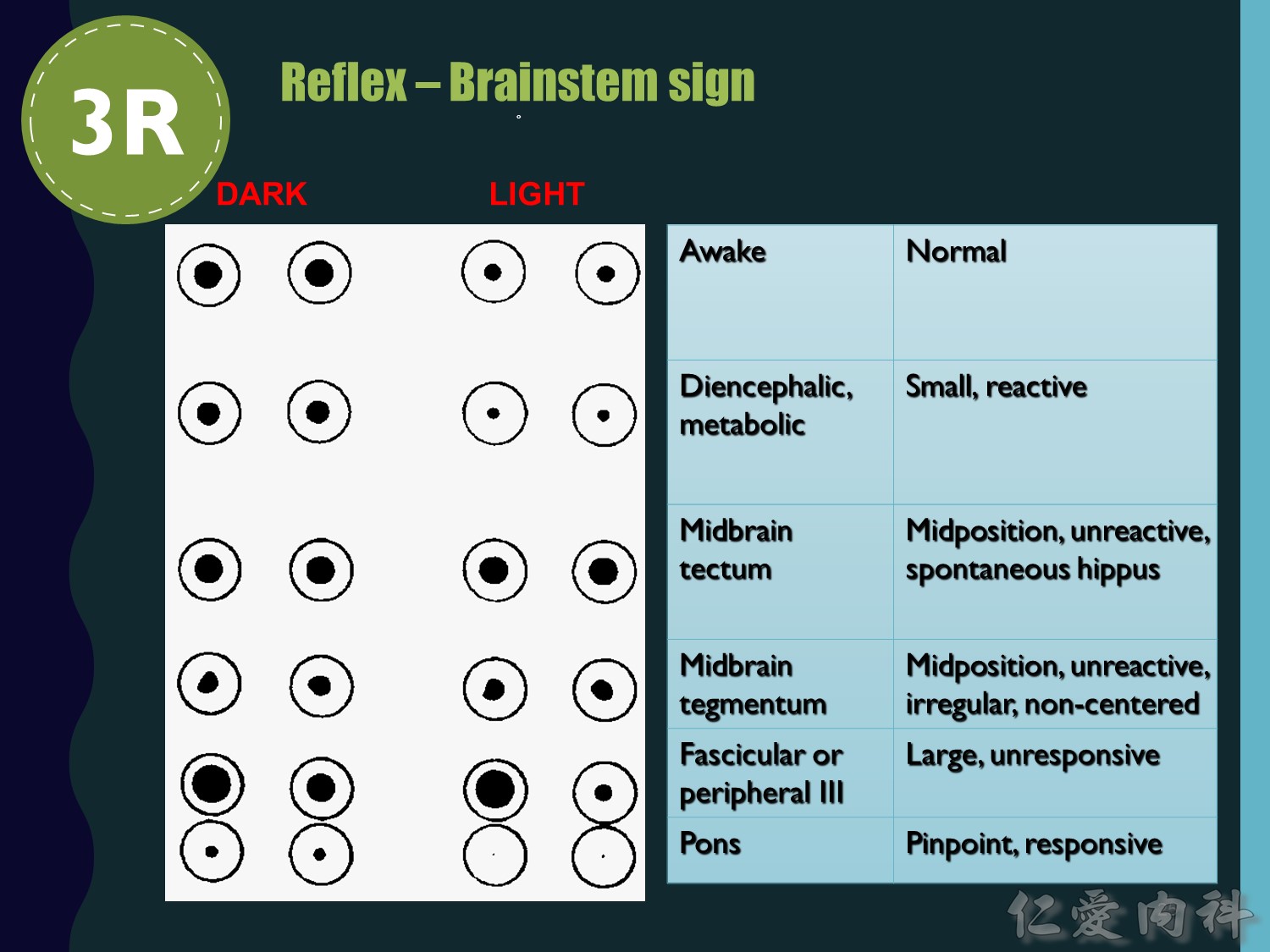
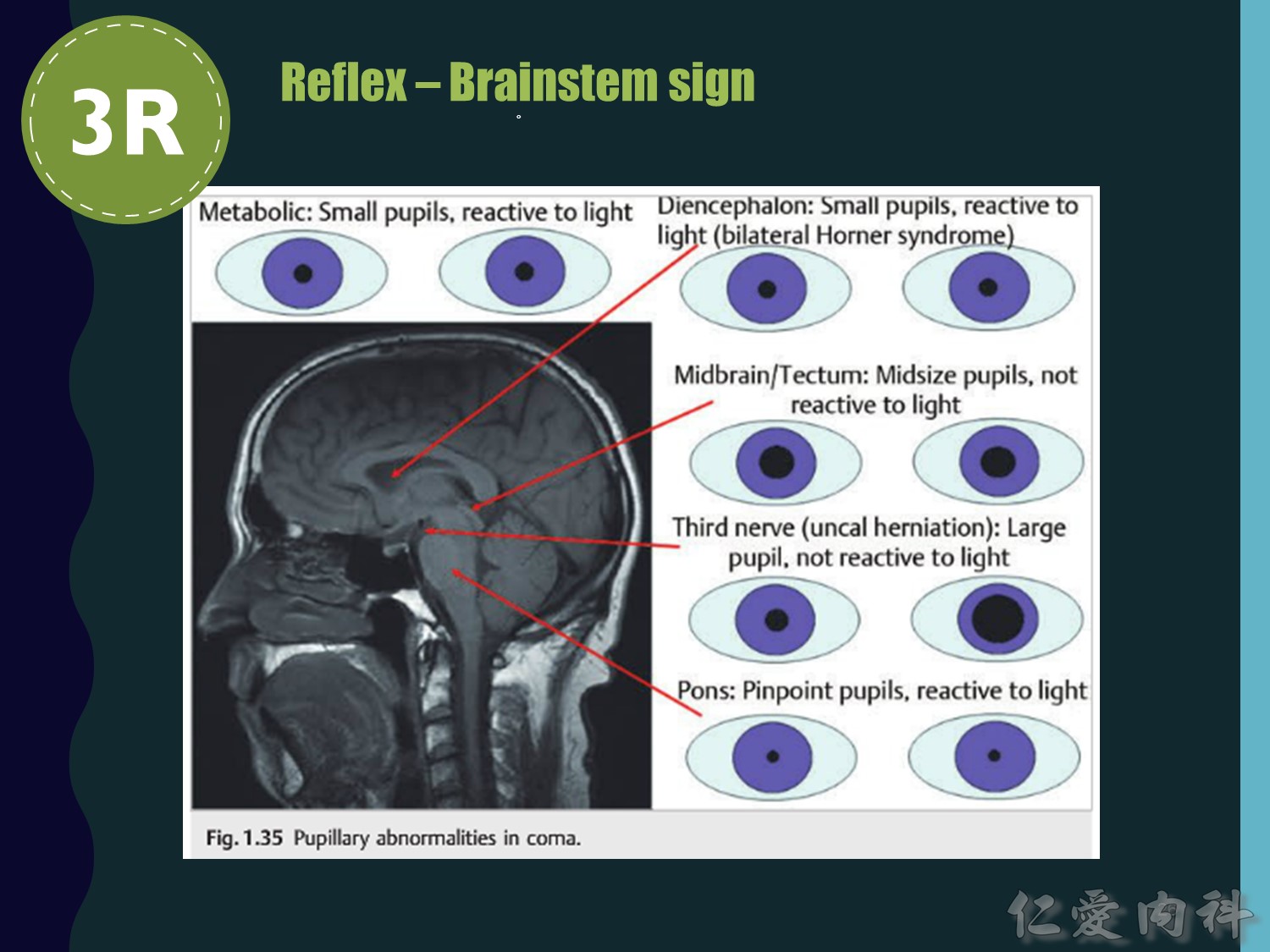
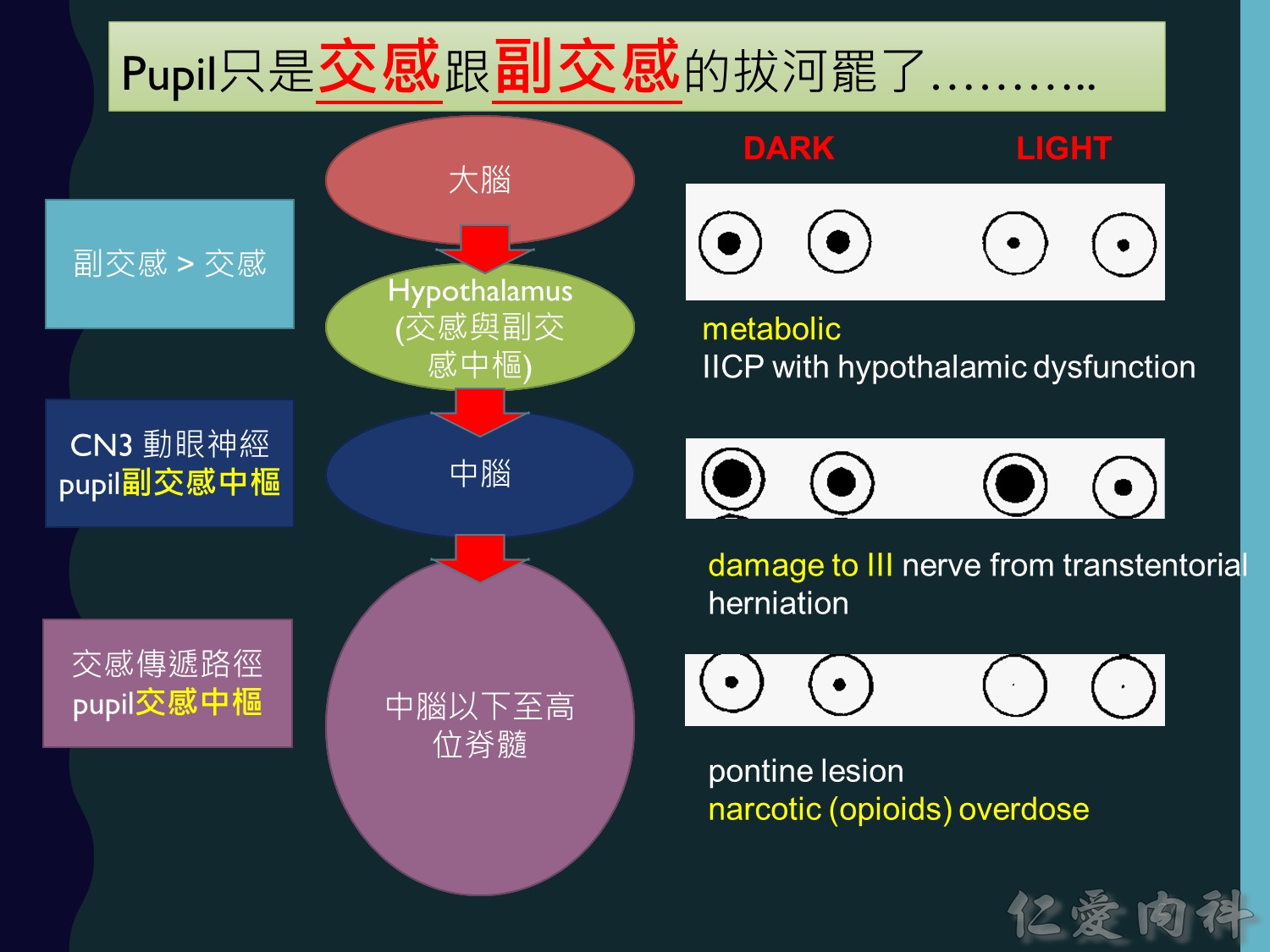
另一個大重點 – pupil 就是 交感副交感的拔河!
1.人體是副交感比較強 所以 metabolic encephalopathy全部影響但副交感比較強所以是miosis
2.Hippus pupil (光照會忽大忽小) 非常嚴重的 metabolic encephalopathy
3.Midbrain 有第三對 cranial nerve (副交感) 所以傷到會dilate
4.midbrain以下是交感,所以傷到會constrict 所以pontine hemorrhage 會 miosis
Harrison:
因為RAS 跟 midbrain 的位置相近 ,故可藉由midbrain dysfunction來localize coma的原因
所以簡單來說 要是有 pupillary light reactivity 以及 eye movement , 可以大致判定coma 是cerebral hemisphere 而不是brainstem
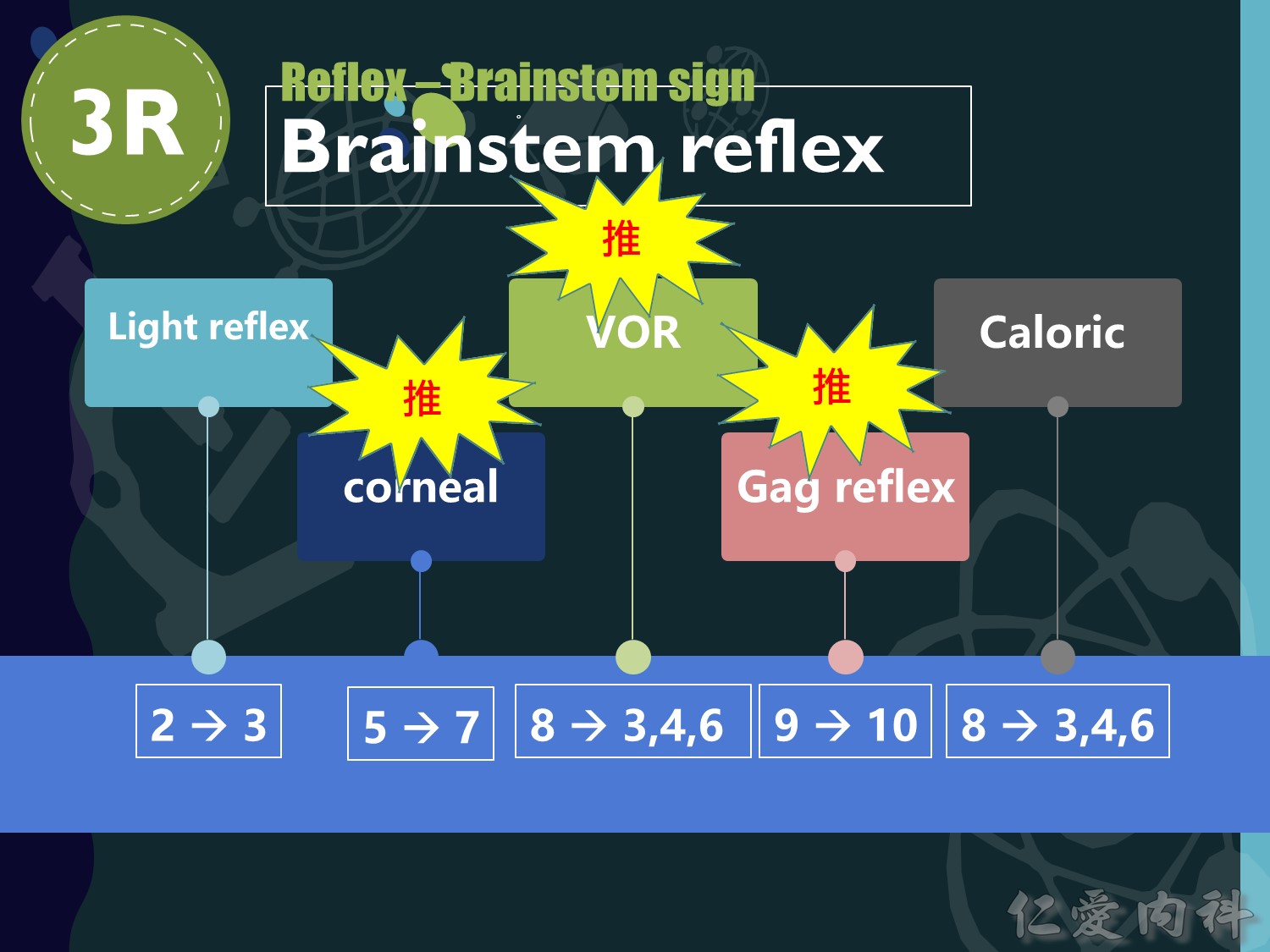
Light reflex 臨床不好用 因為病人一堆cataract 很多老人的reflex也很頓
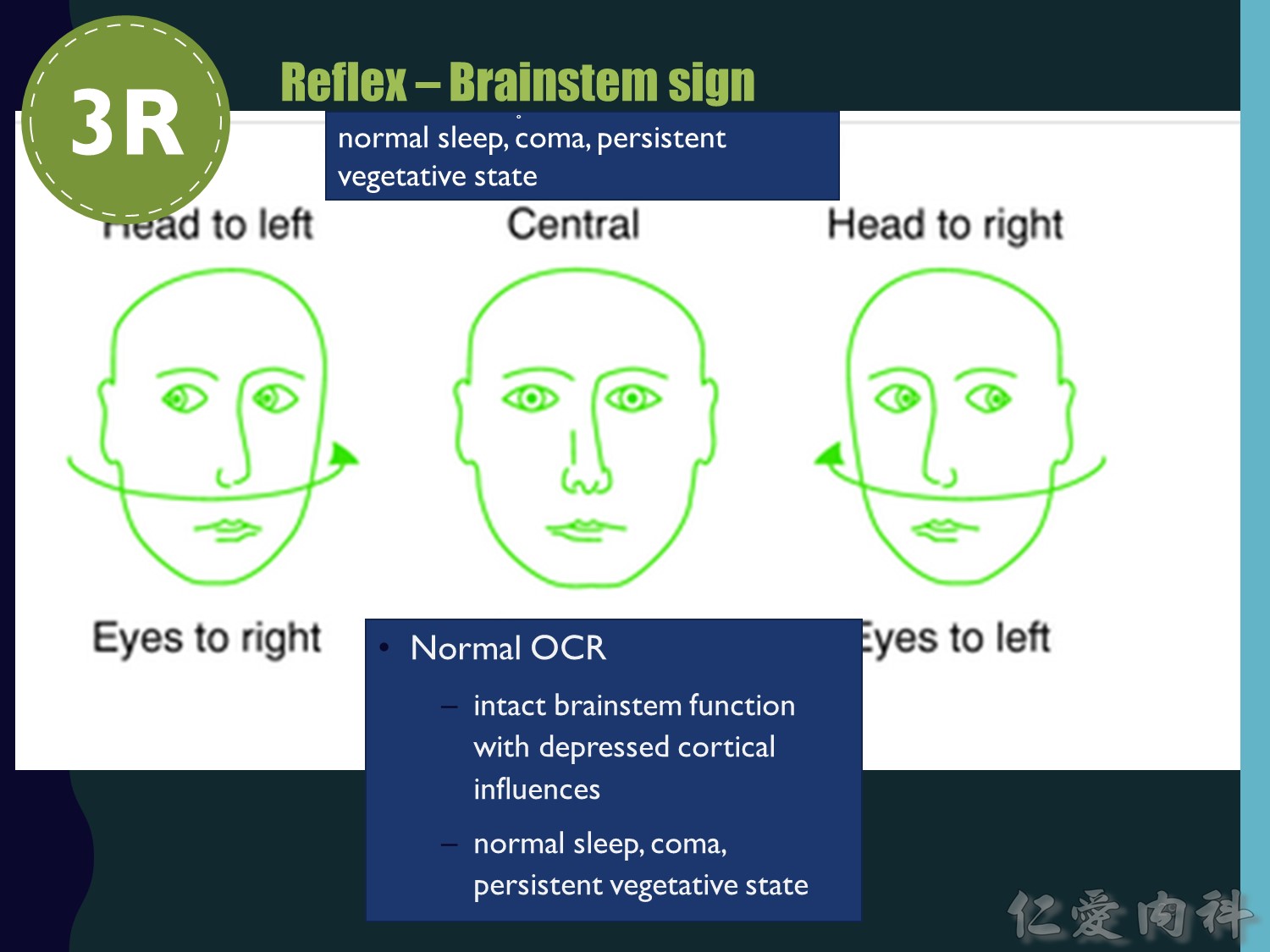
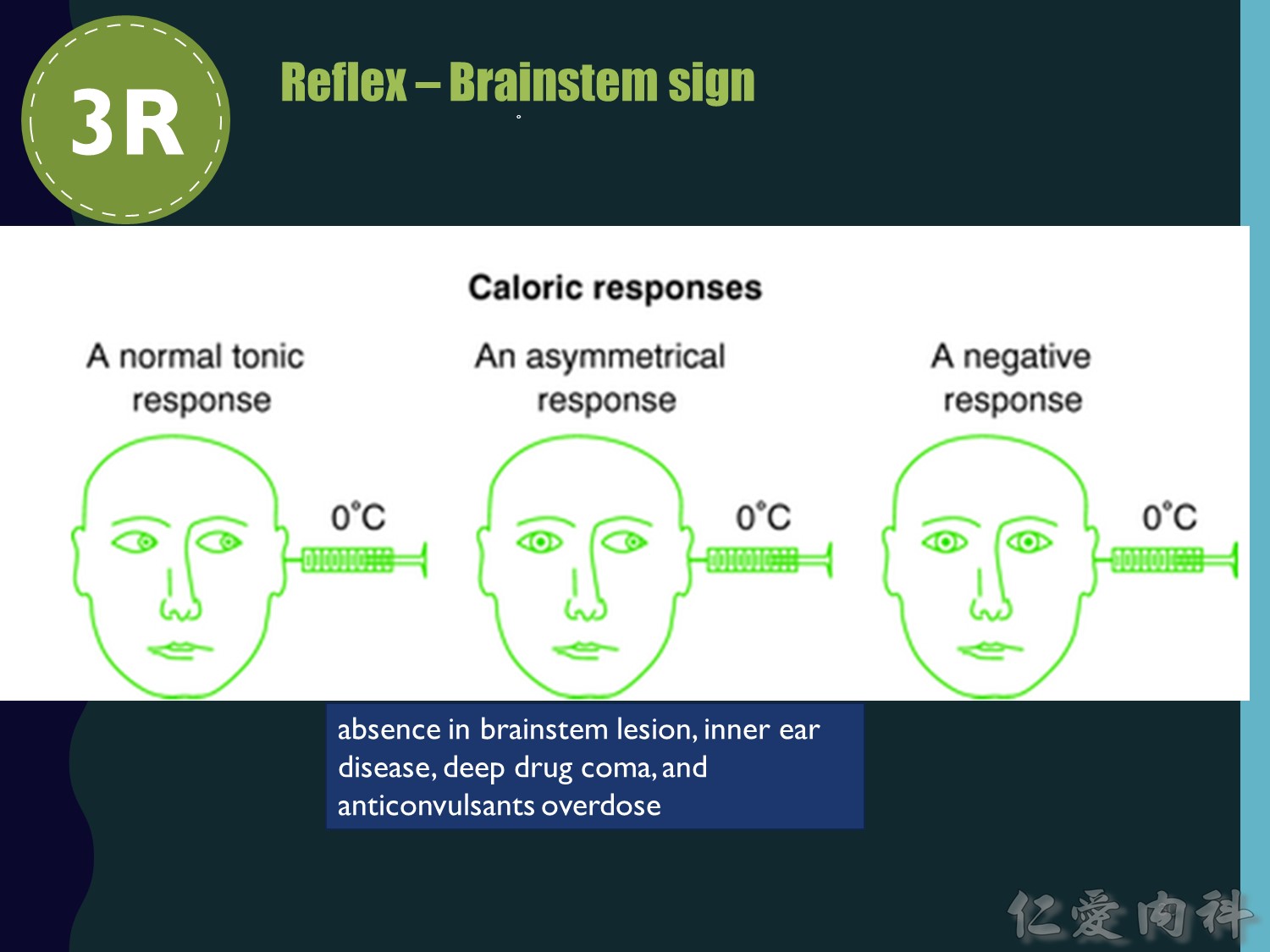
比較推薦的 還是 corneal VOR, Gag
VOR (搖得出來算是doll eye positive, 是正常的)
-意識清醒 要 要搖快一點 ,因為清醒的人會有 cortex的 reflex
-意識不清搖慢一點
Gag – 請護理師抽痰
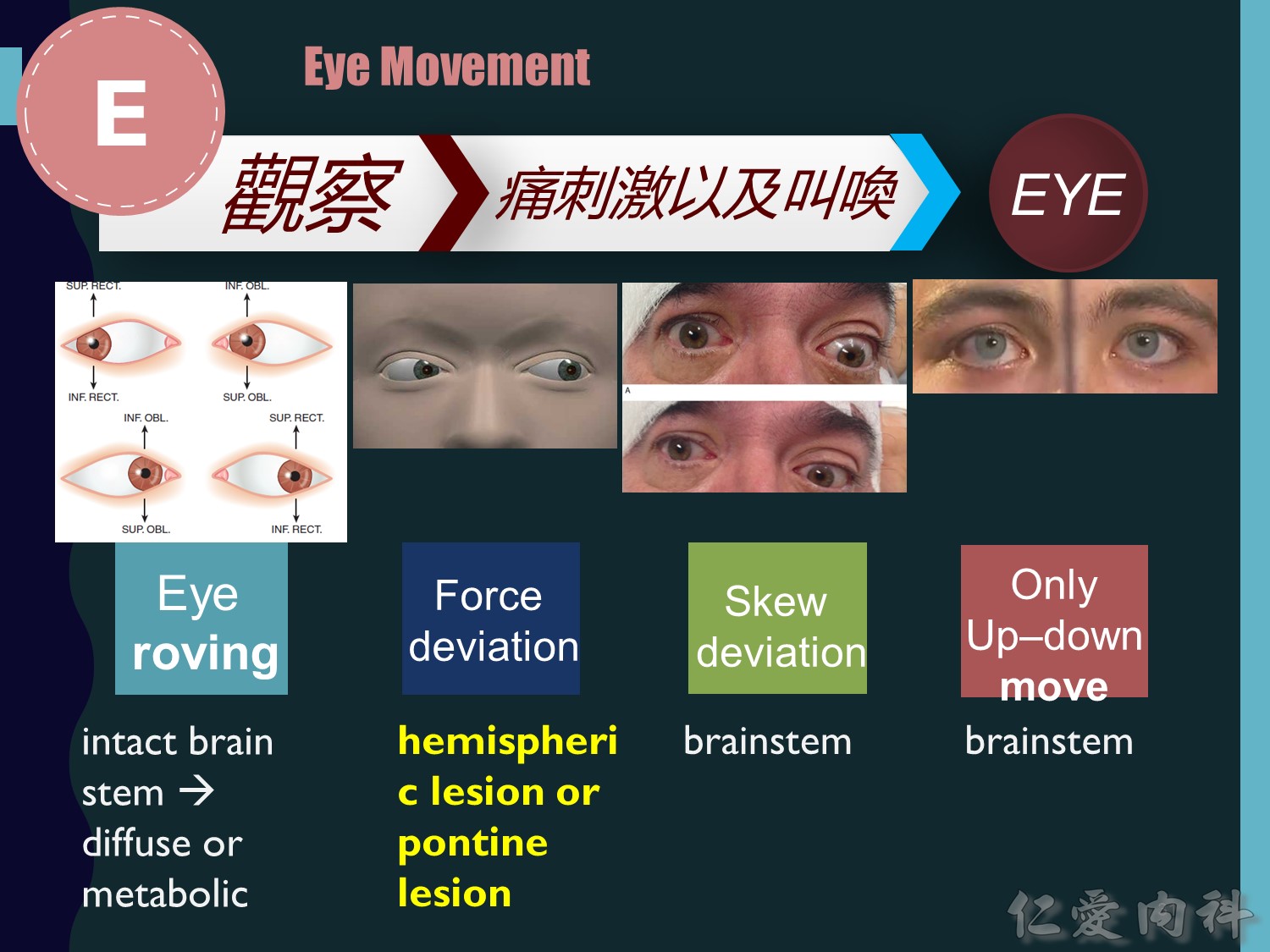
. EYE roving- 眼睛看左看右- intact brain stem
. Force deviation – 大同橋異 (如果是右側大腦問題眼睛看右,如果是右側橋腦問題眼睛看左)
. Skew deviation – 眼睛脫窗- brainstem lesion
. Only up-down move – brainstaem lesion
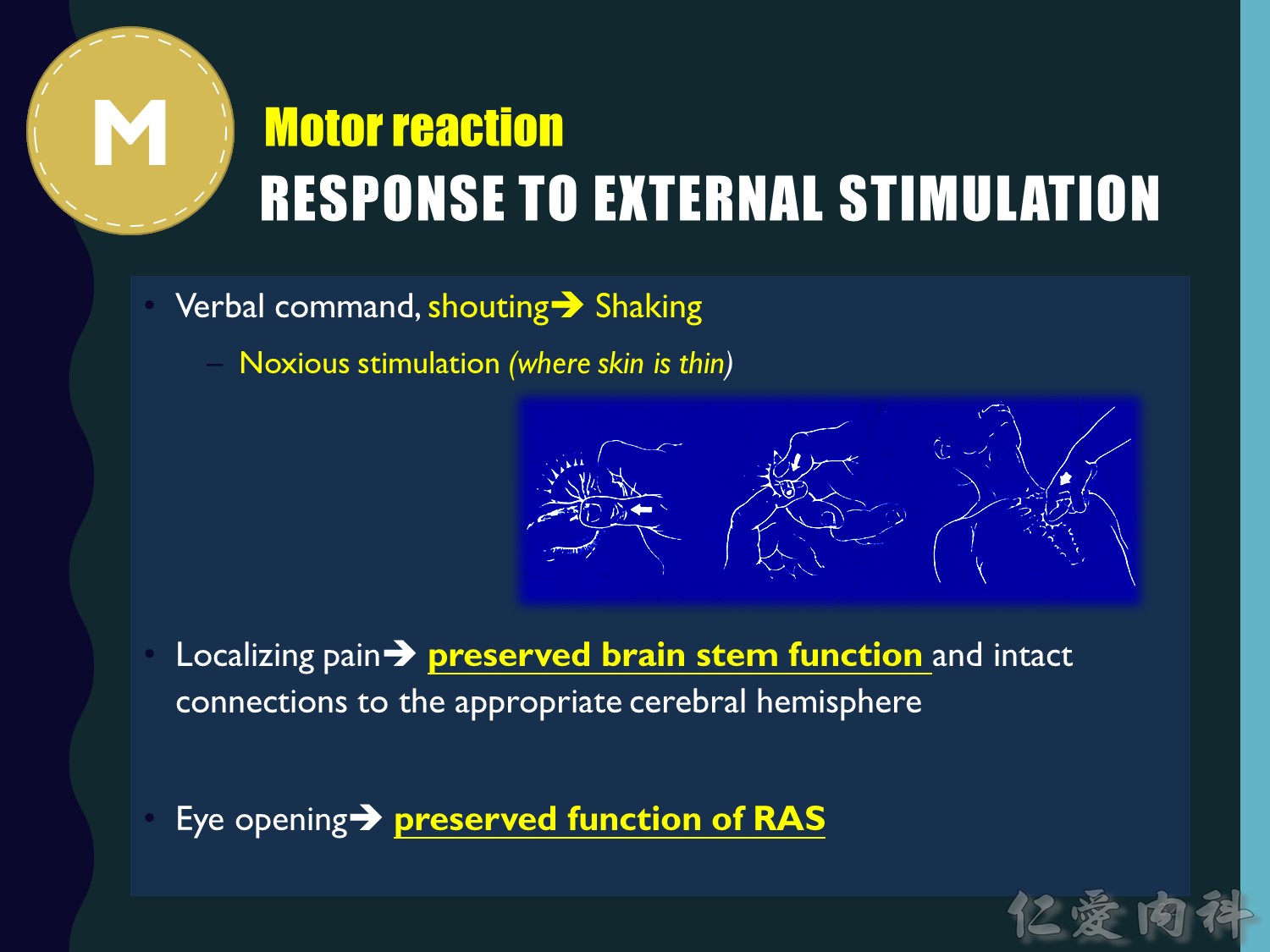
如果可以對疼痛刺激可以有反應 代表 腦幹”功能”正常 (還是有可能有損傷)
如果叫了眼睛可睜開 – RAS 正常
M2 M3 比較有 localization的意義
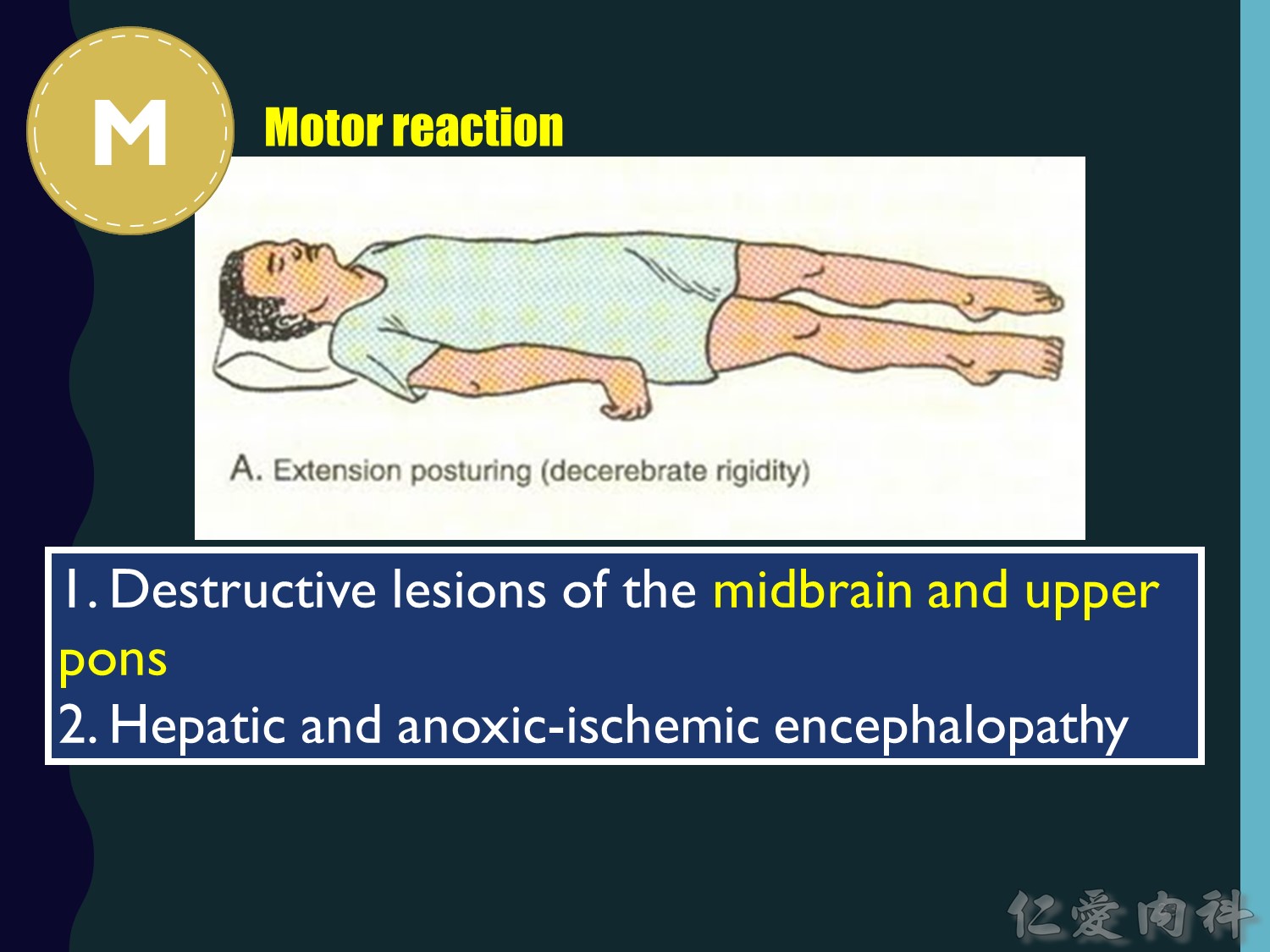
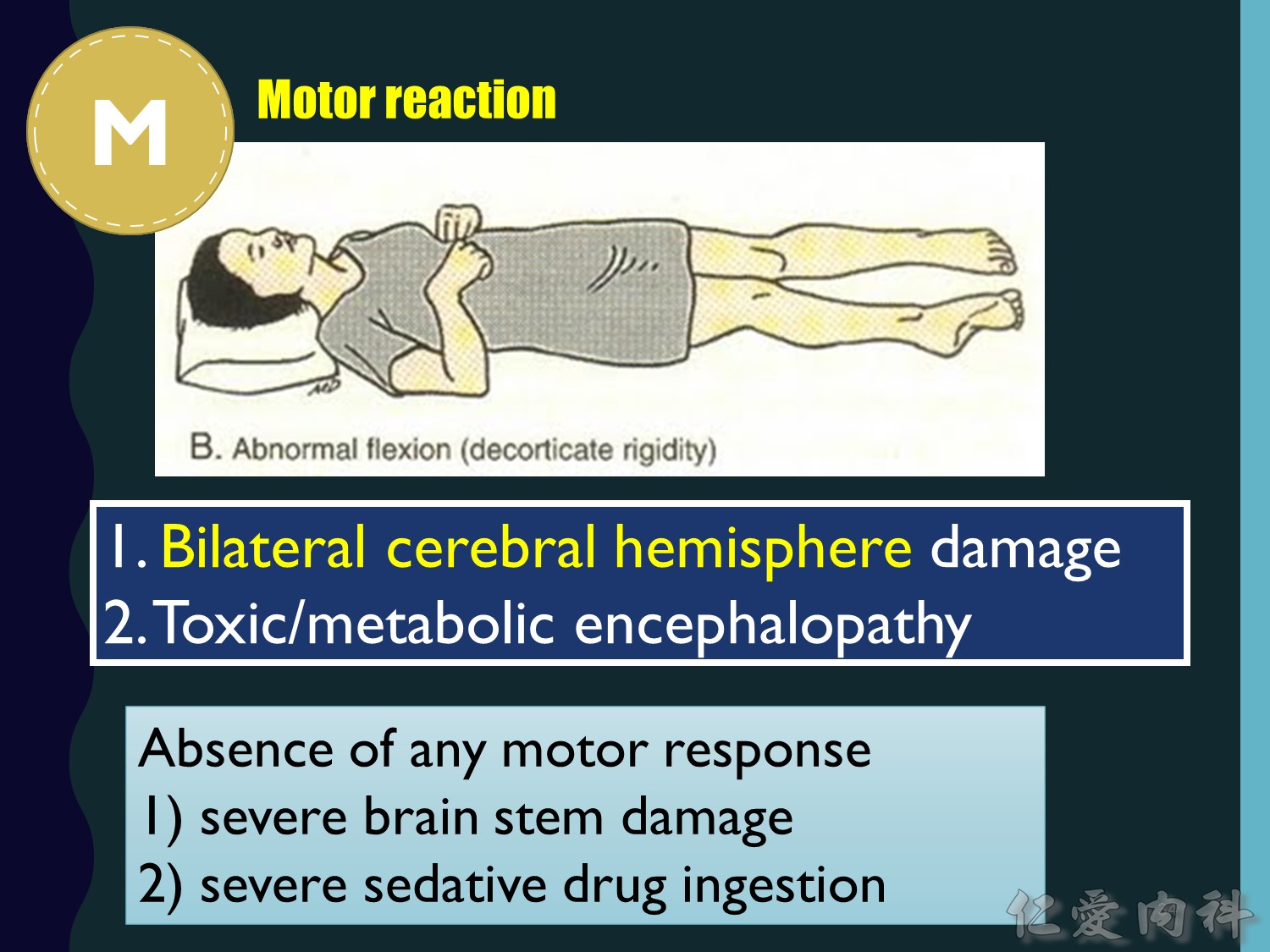
注意!
如果對痛完全無反應 除了嚴重腦損傷之外 sedative也可以

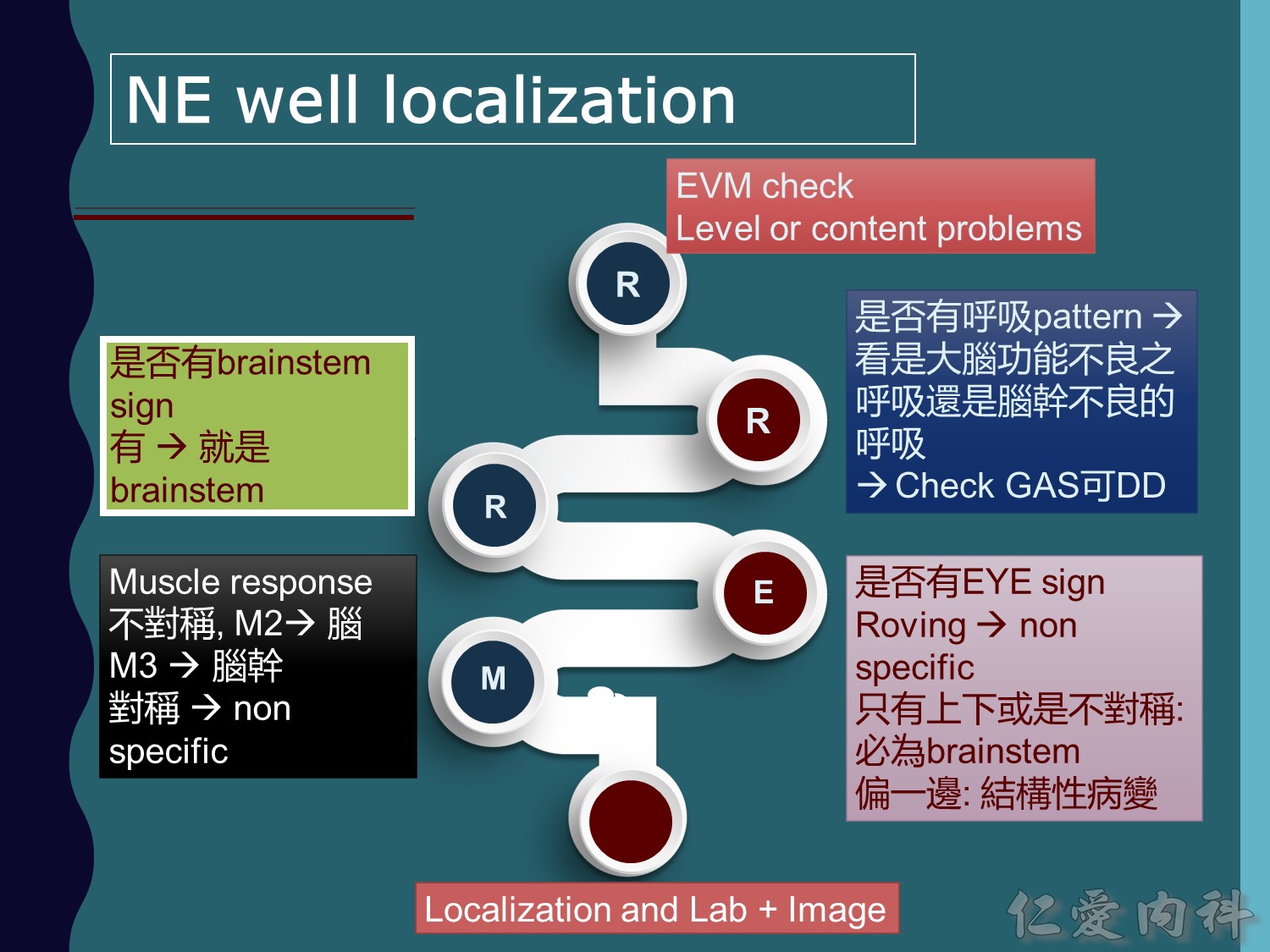
Coma 的 assessment 要3REM綜合評估
而不是 一個 neurological finding 對應一個 location
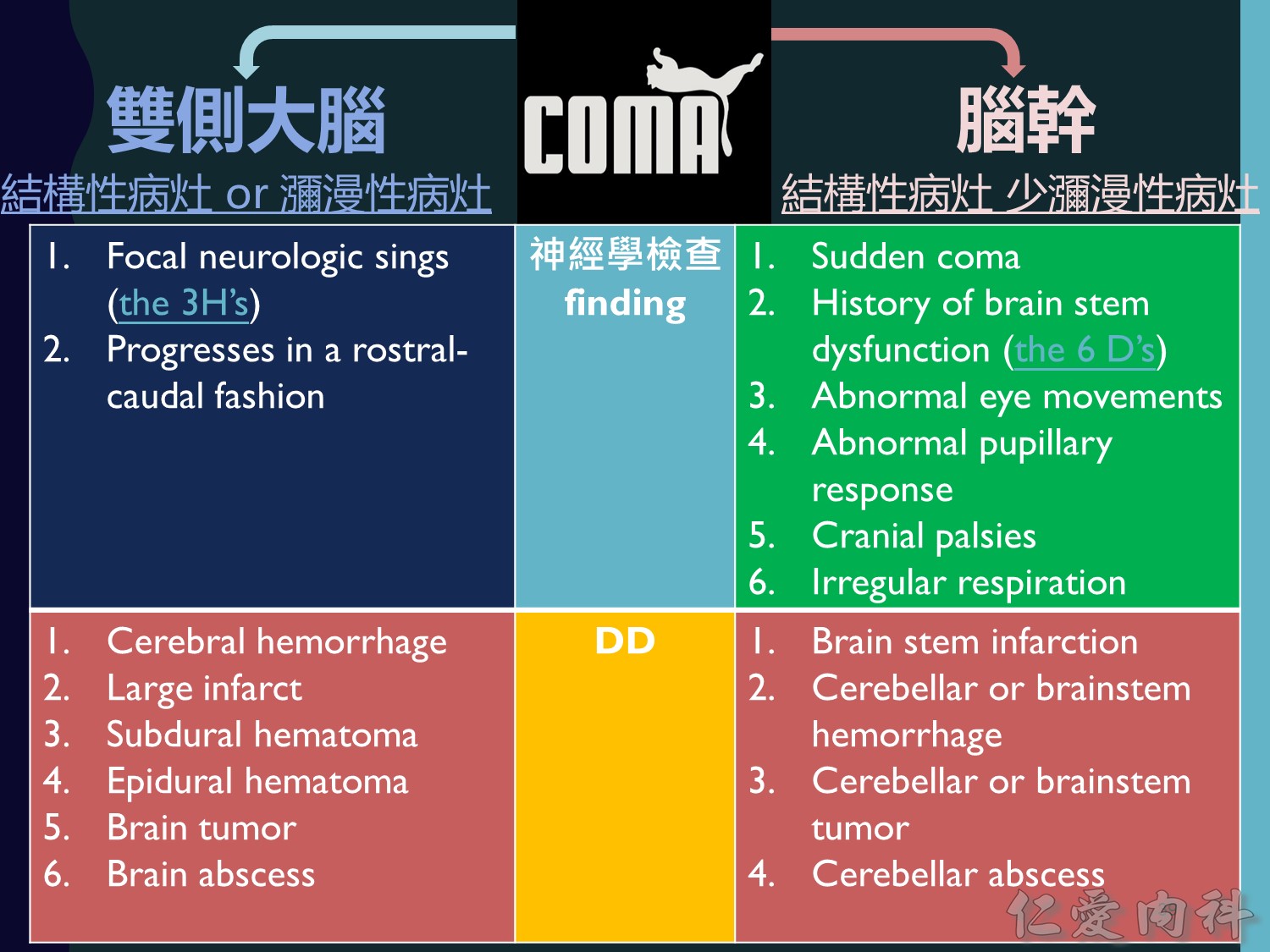
Harrison 強調
– 很多durg/toxin會同時影響大腦跟腦幹 所以雙側大腦跟腦幹的sign都有常常會被誤認成腦幹結構性問題 謹記!
– 大部分的medical causes都不用影像診斷,如果去照了可能還會誤診,例: CT:small SDH or old stroke 但其實有吃BZD
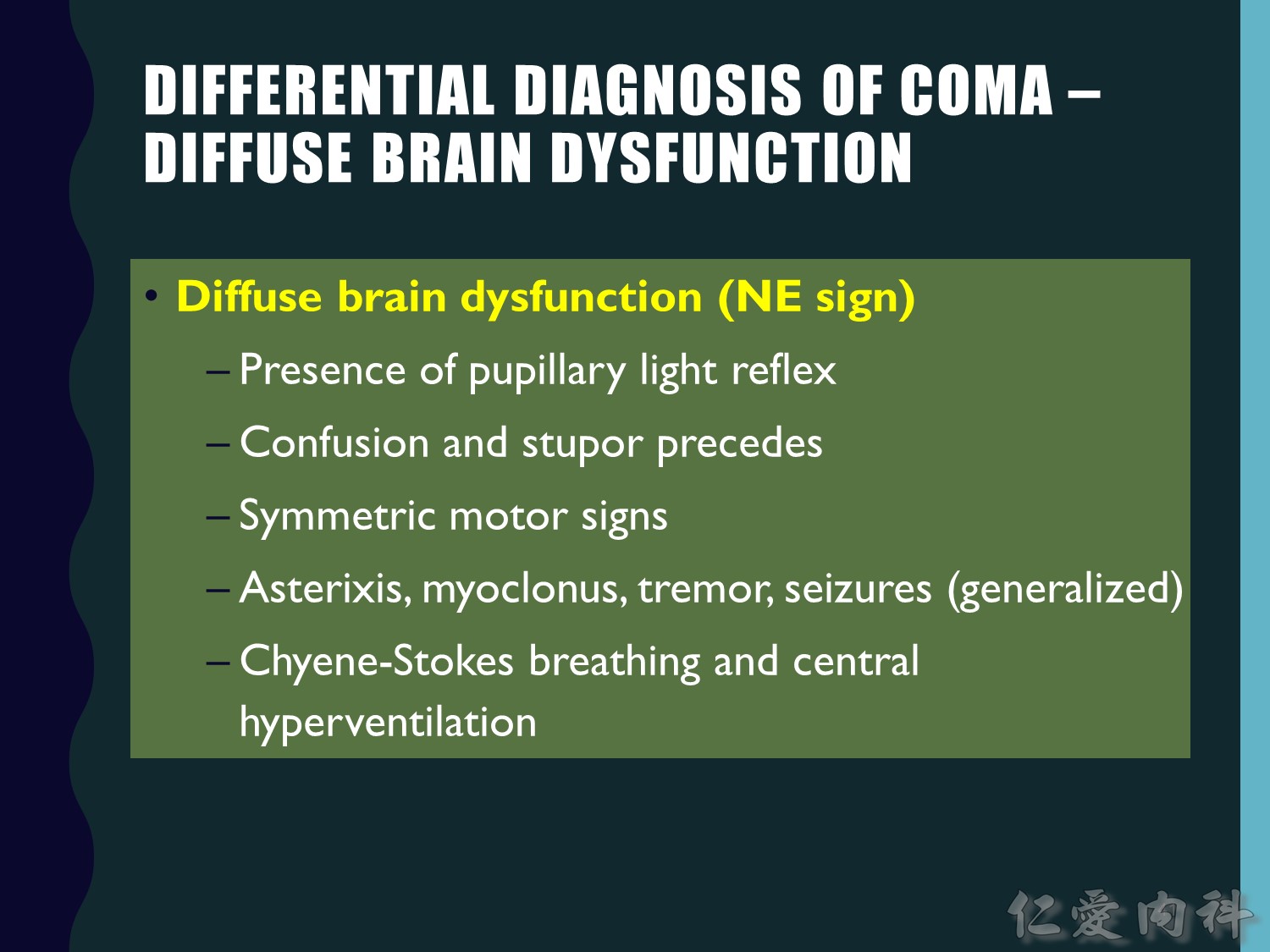
Diffuse brain dysfunction = metabolic encephalopathy
Cerebral neuron 完全仰賴
1.CBF (cerebral blood flow)
2.O2 and glucose delivery
要是 CBF interrupted
Glucose store可以撐2分鐘
Oxygen store 可以撐8-10秒
– 別忘了抽Glucose
– 有沒有吃BZD
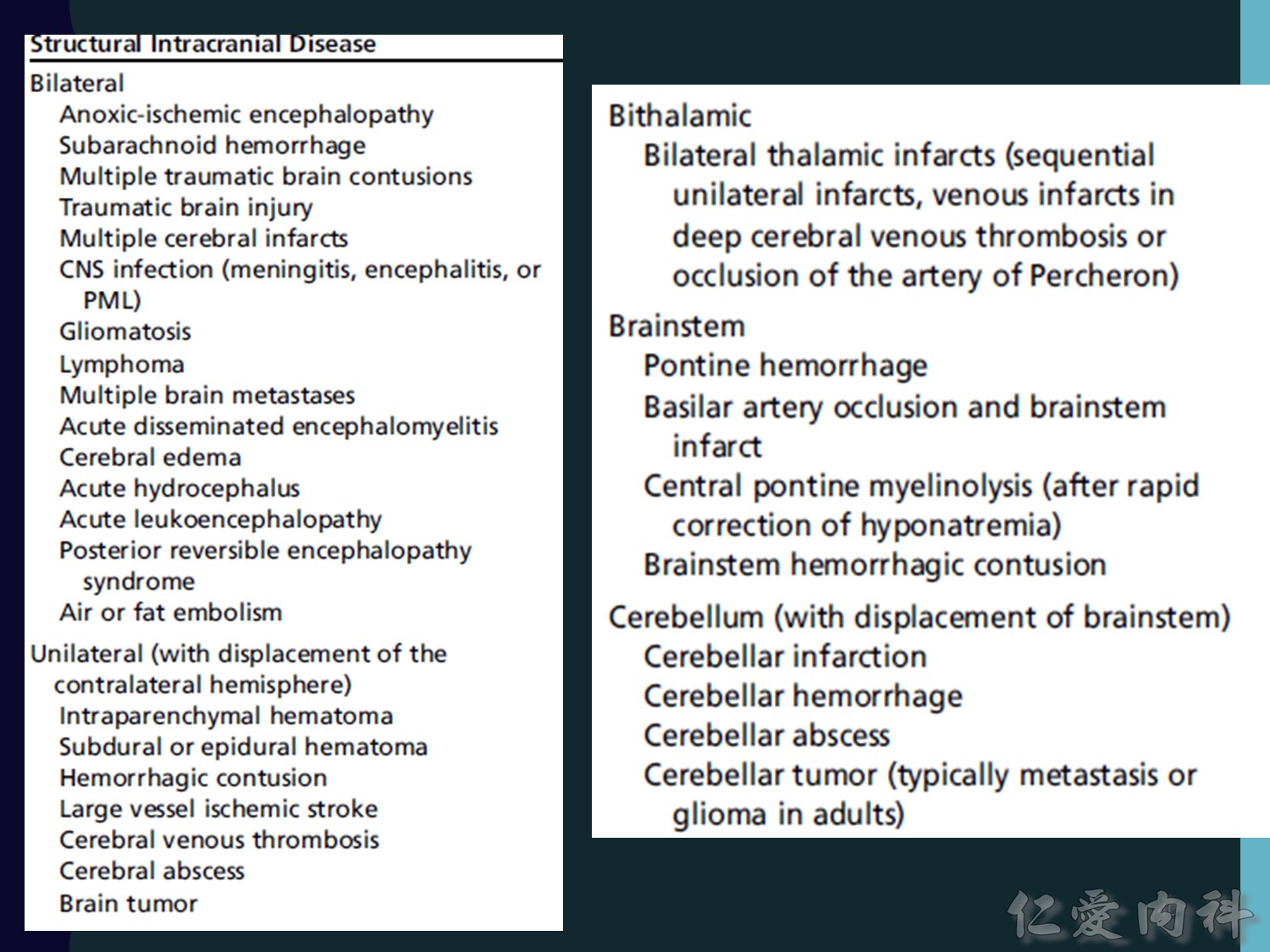
有很多口訣 可背 AEIOU TIPS 的細項就不贅述了,我附一些Harrison的Differential
1.Without focal sign- metabolic and toxic encephalopathy
2.With focal sign – stroke, cerebral hemorrhage
3.Meningitis syndrome (fever, stiff neck, excess cells in spinal fluid)- bacterial meningitis, SAH, encephalitis
時間的分法
Suddden- cardiac arrest, epilepsy, basilar artery occlusion, drug ingestion, cerebral hemorrhage, trauma
Subacutely – preexisting medical or neurologic problem, secondary brain swelling surrounding tumor or cerebral infarction
**常見的中風不會Coma, 但大片infarction之後的edema 導致的Mass effect有可能
腦血管的病變導致的COMA 有五個
1.Basal ganglia and thalamic hemorrhage
2.Pontine hemorrhage(sudden, pinpoint, loss of corneal VOR reflex, hyperventilation)
3.Cerebellar hemorrhage (occipital headache, vomiting, inability to stand, 視出血程度壓到brainstem多寡來決定coma的快慢)
4.Basilar artery thrombosis (diplopia, dysarthria, vomiting, loss of corneal VOR reflex, asymmetric limb paresis)
5.Subarachnoid hemorrhage(sudden severe headache and vomiting followed by coma)