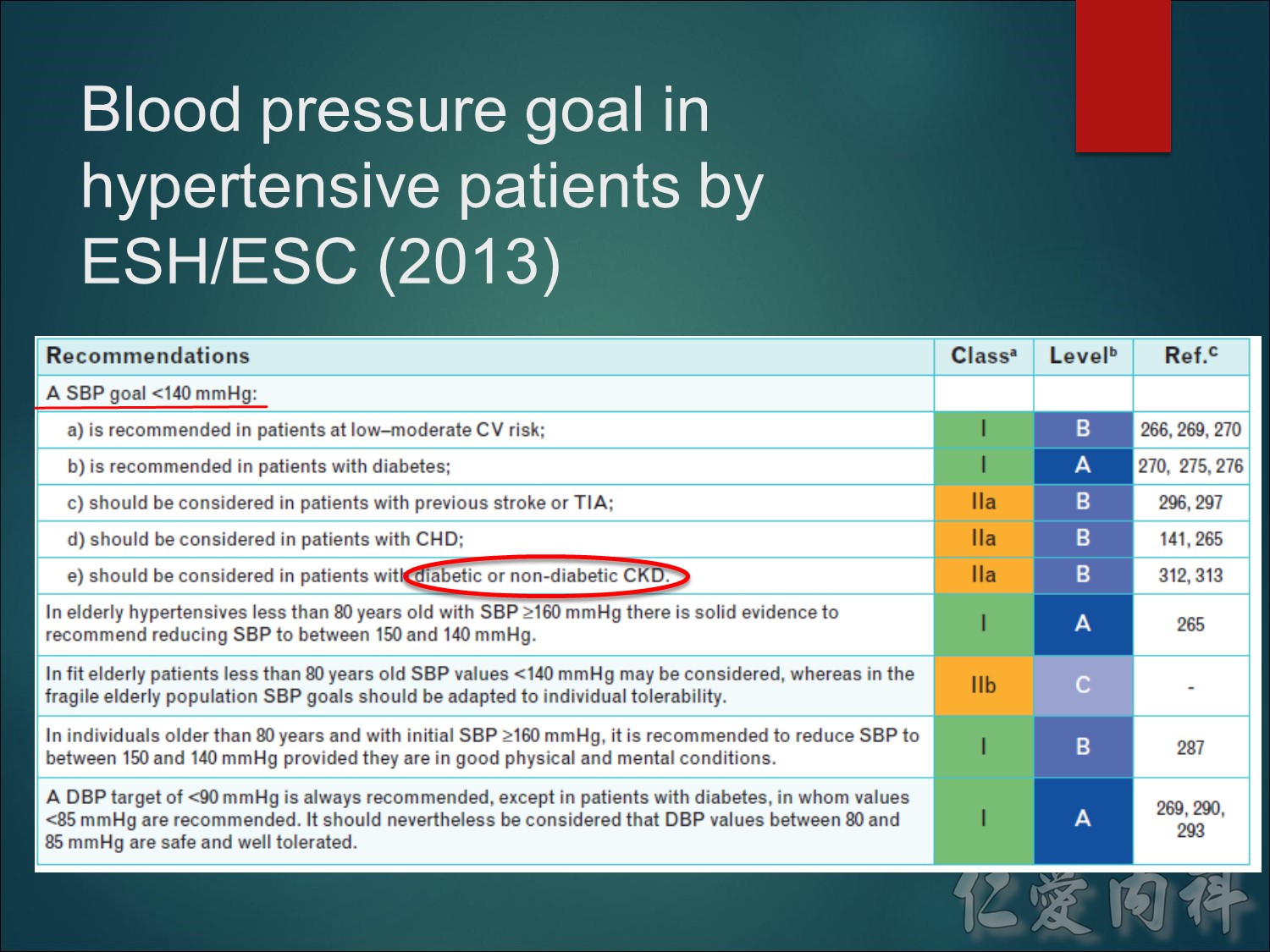
最新版WHO/ISH高血壓規範也於2003年出版,自從一九九九年出版WHO/ISH高血壓管理規範後,現在已經有更多證據支持收縮壓140 mmHg的標準足以構成「低危險群」患者的條件。WHO/ISH和ESH/ESC的定義非常類似。
註:高危險群病患
至於其他規範,WHO/ISH 2003的建議是針對心血管高危險群病患,例如糖尿病患者提供較積極的血壓目標。
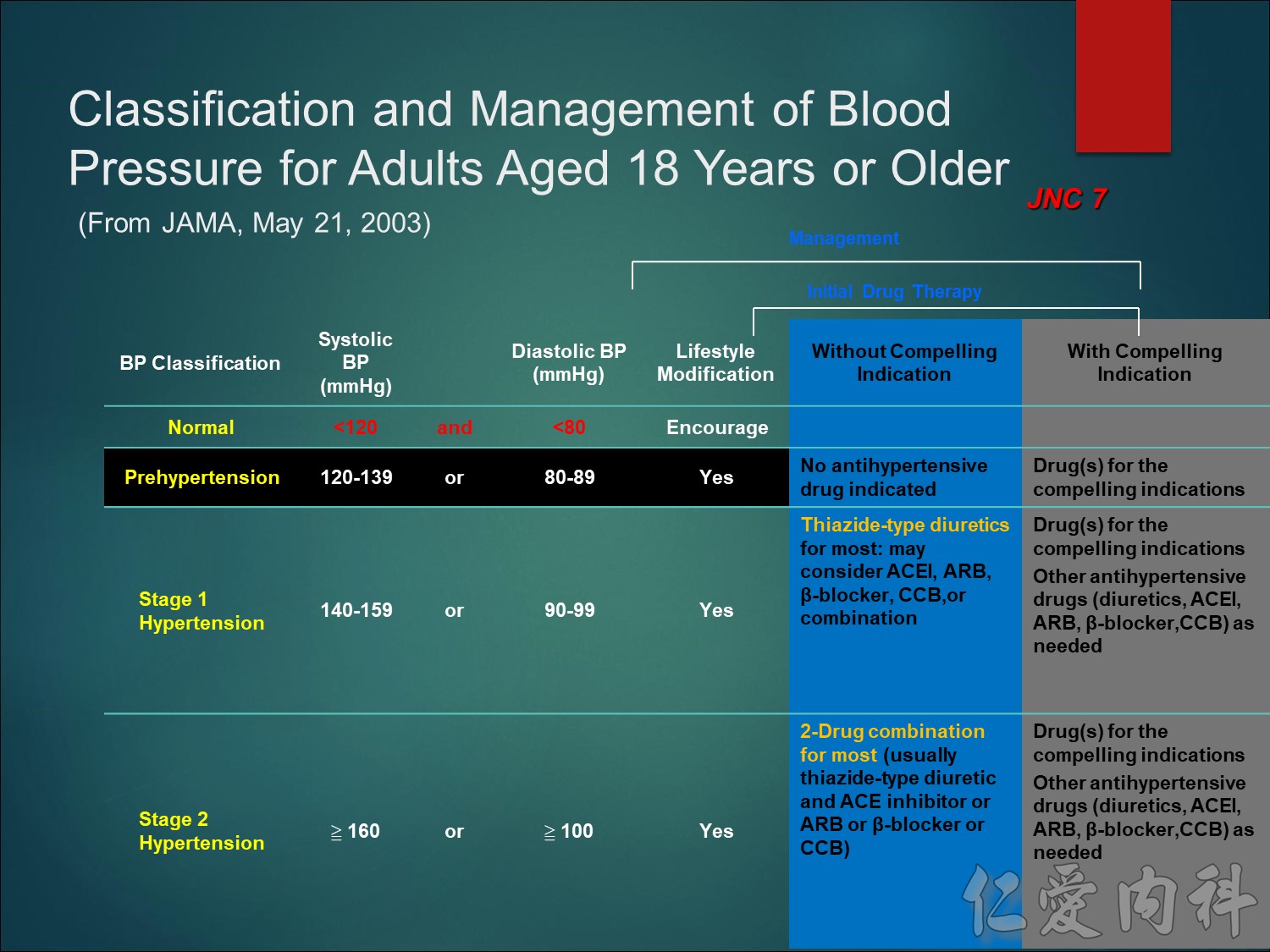
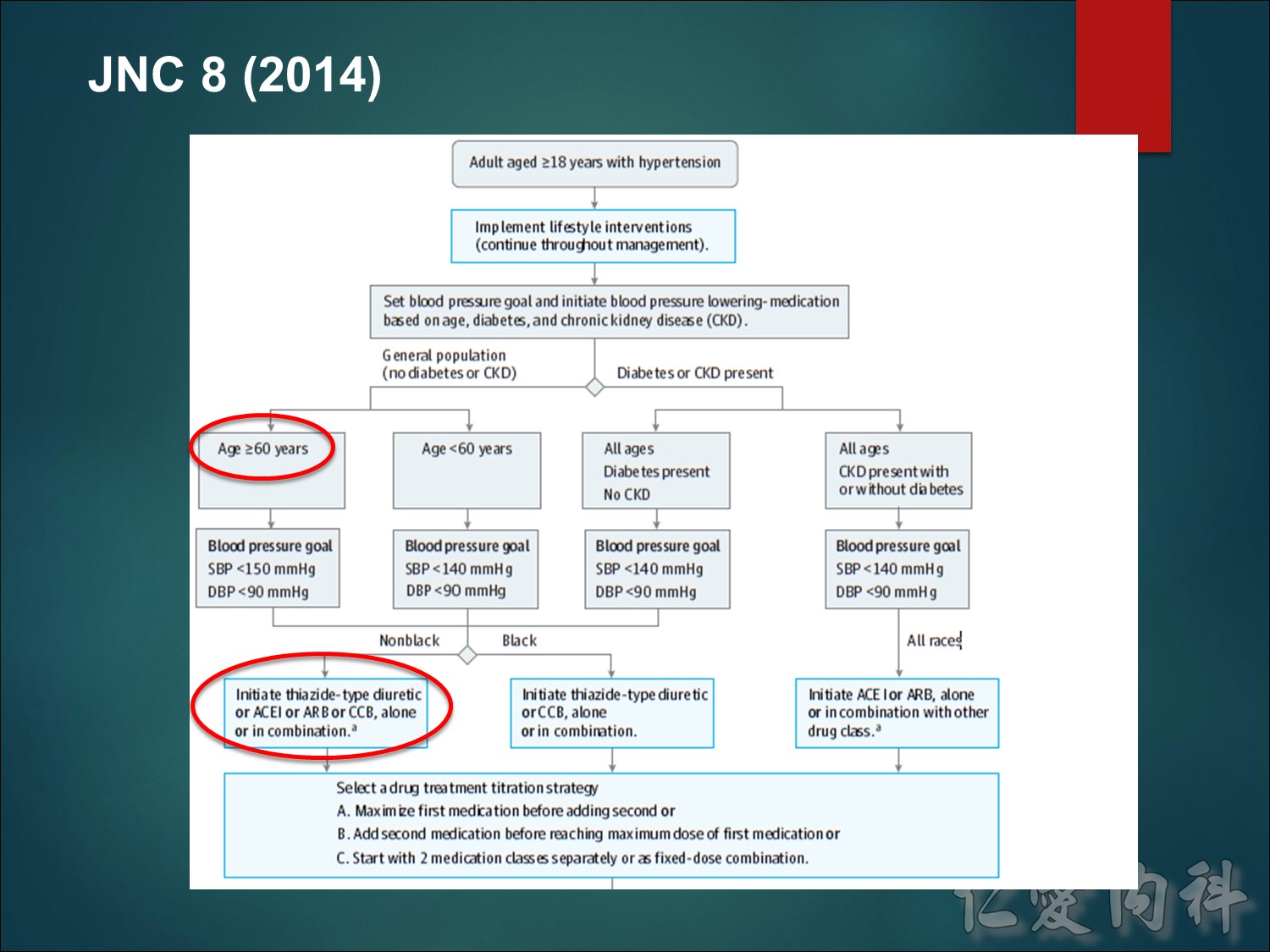
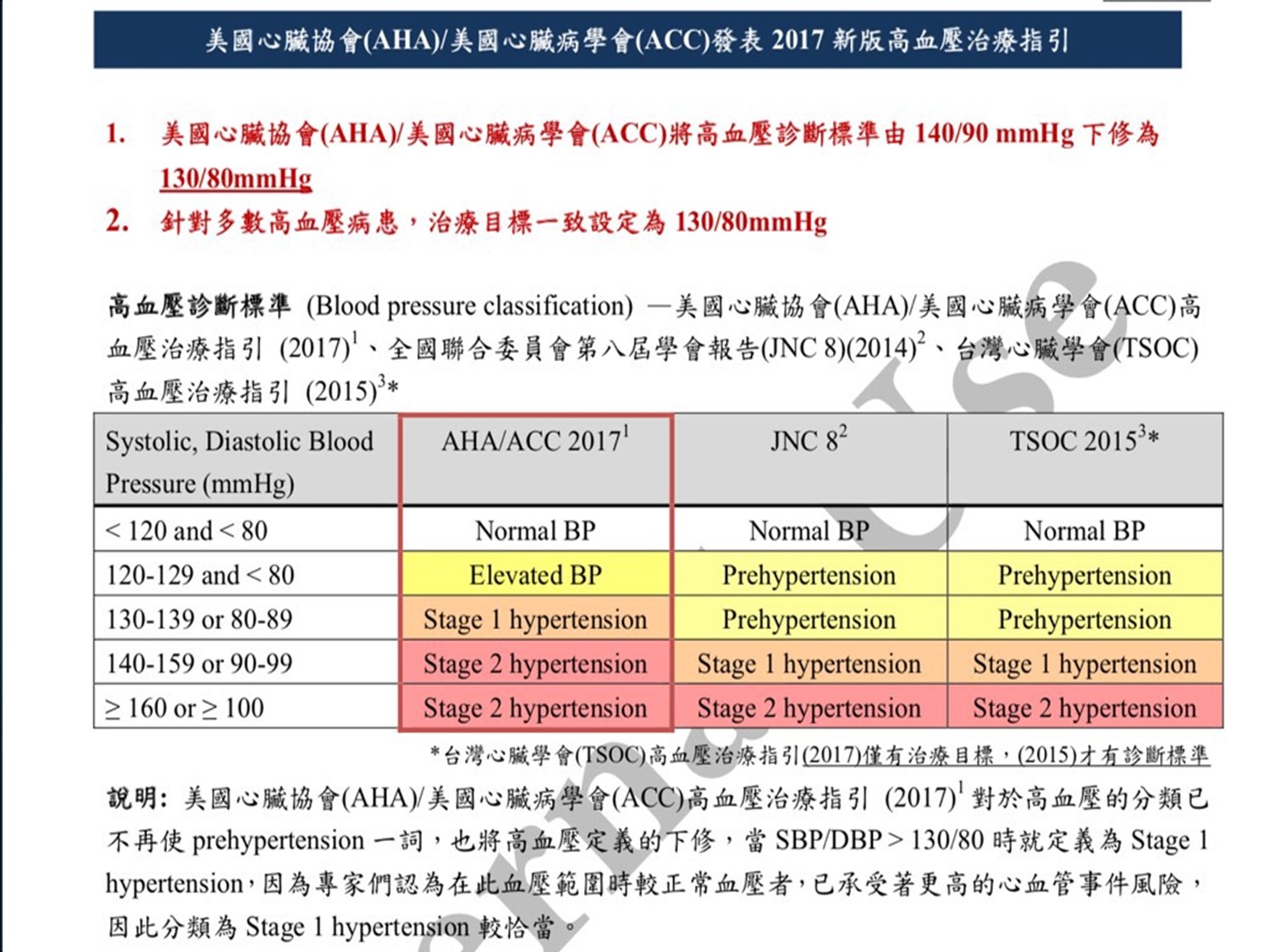
在 JNC 7中,新規劃了 prehypertension(高血壓前期),而 stages 2 and 3 HTN 被合併為一級
This slide details the treatment path recommended by the JNC VII guidelines.
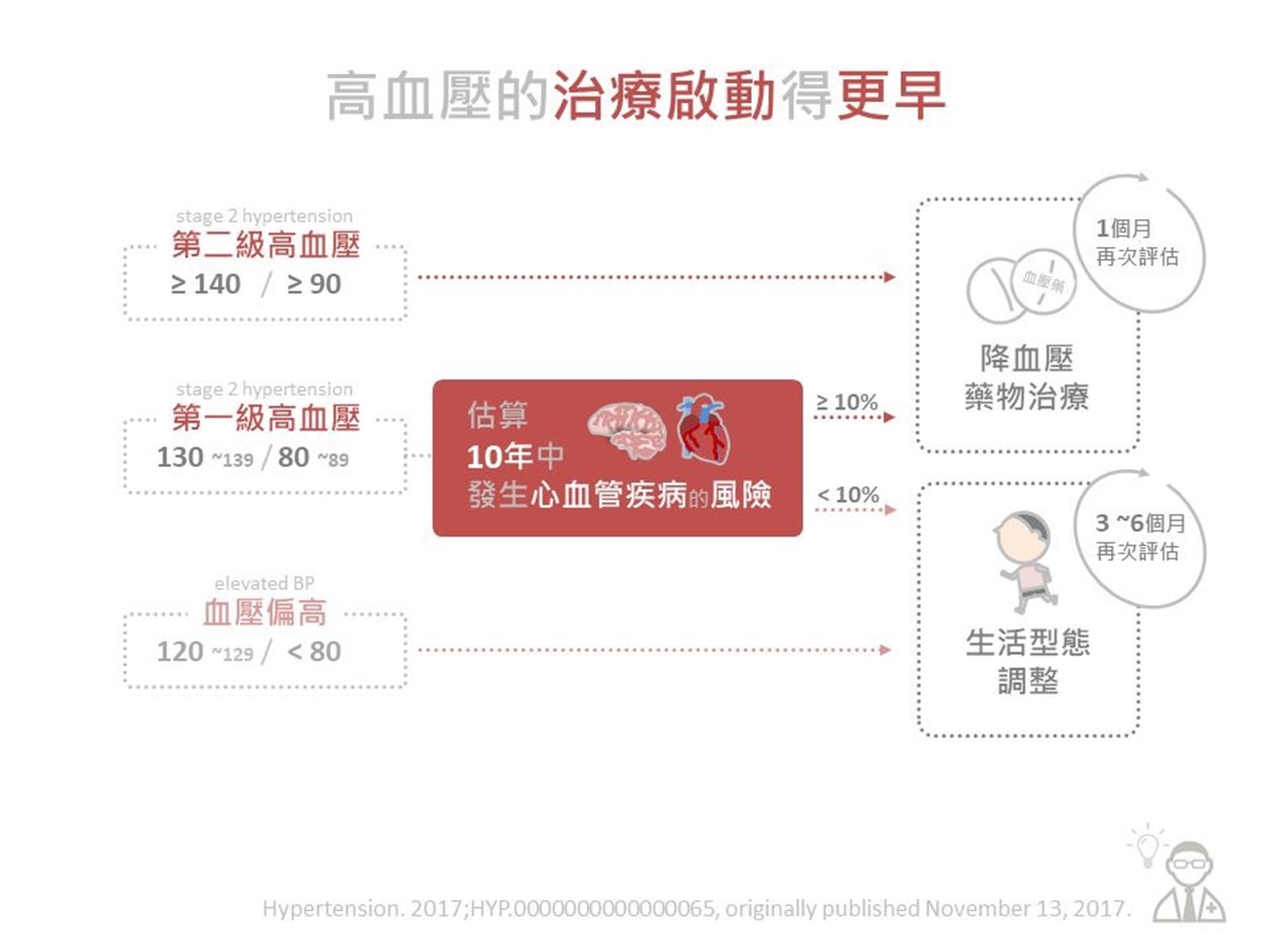
As shown, treatment of hypertension begins with implementing lifestyle changes; this is followed by pharmacologic treatment if BP target levels are not reached.
Compelling indications refer to co-morbidities, such as heart failure, post-myocardial infarction, at high risk of coronary disease, diabetes, and chronic kidney disease.
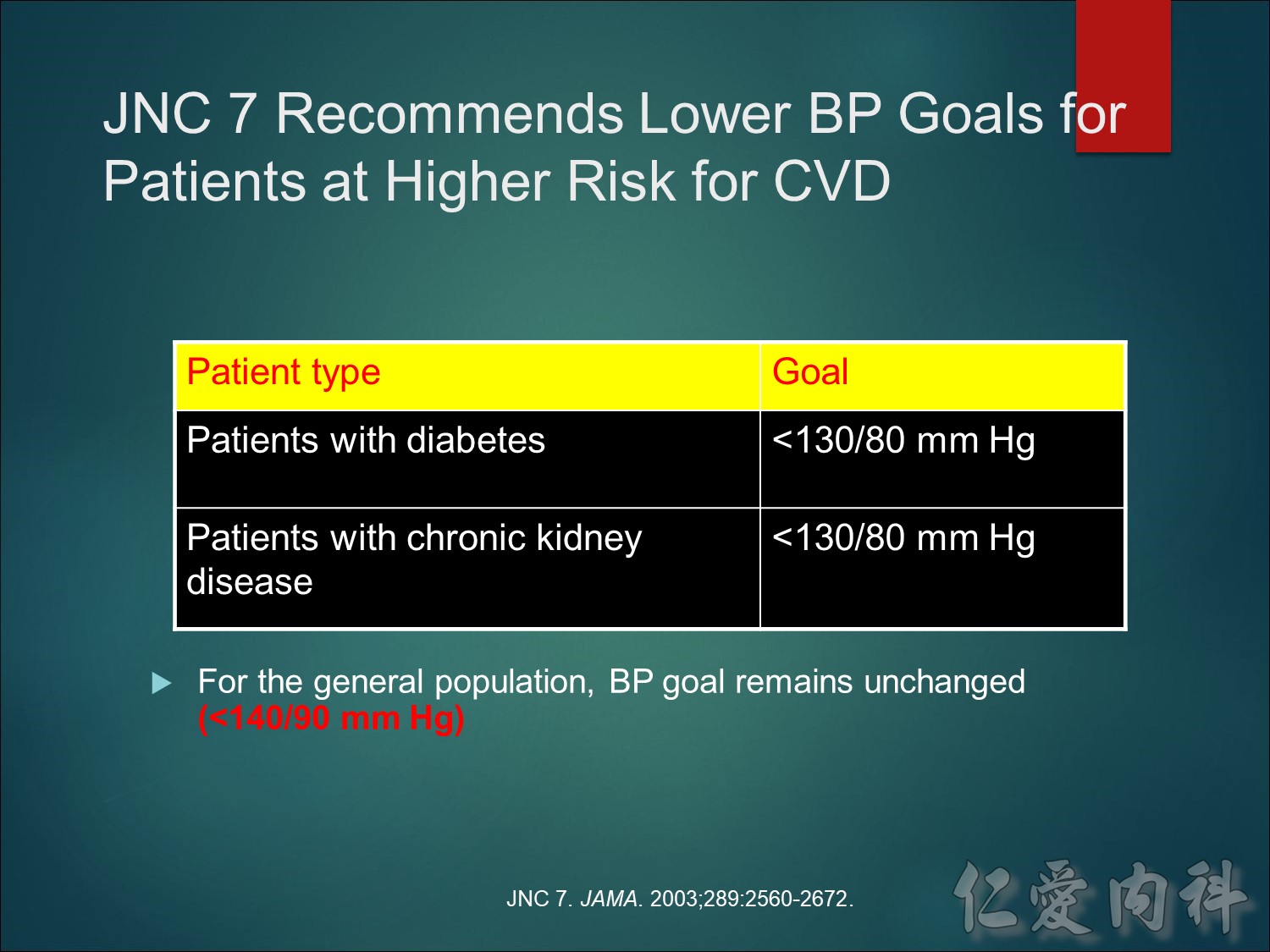
JNC 7 provides new guidelines for prevention and management of hypertension.
The BP goal for individuals without substantial comorbidity is <140/90 mm Hg.
Patients with diabetes or chronic renal failure should aim for a BP <130/80 mm Hg.
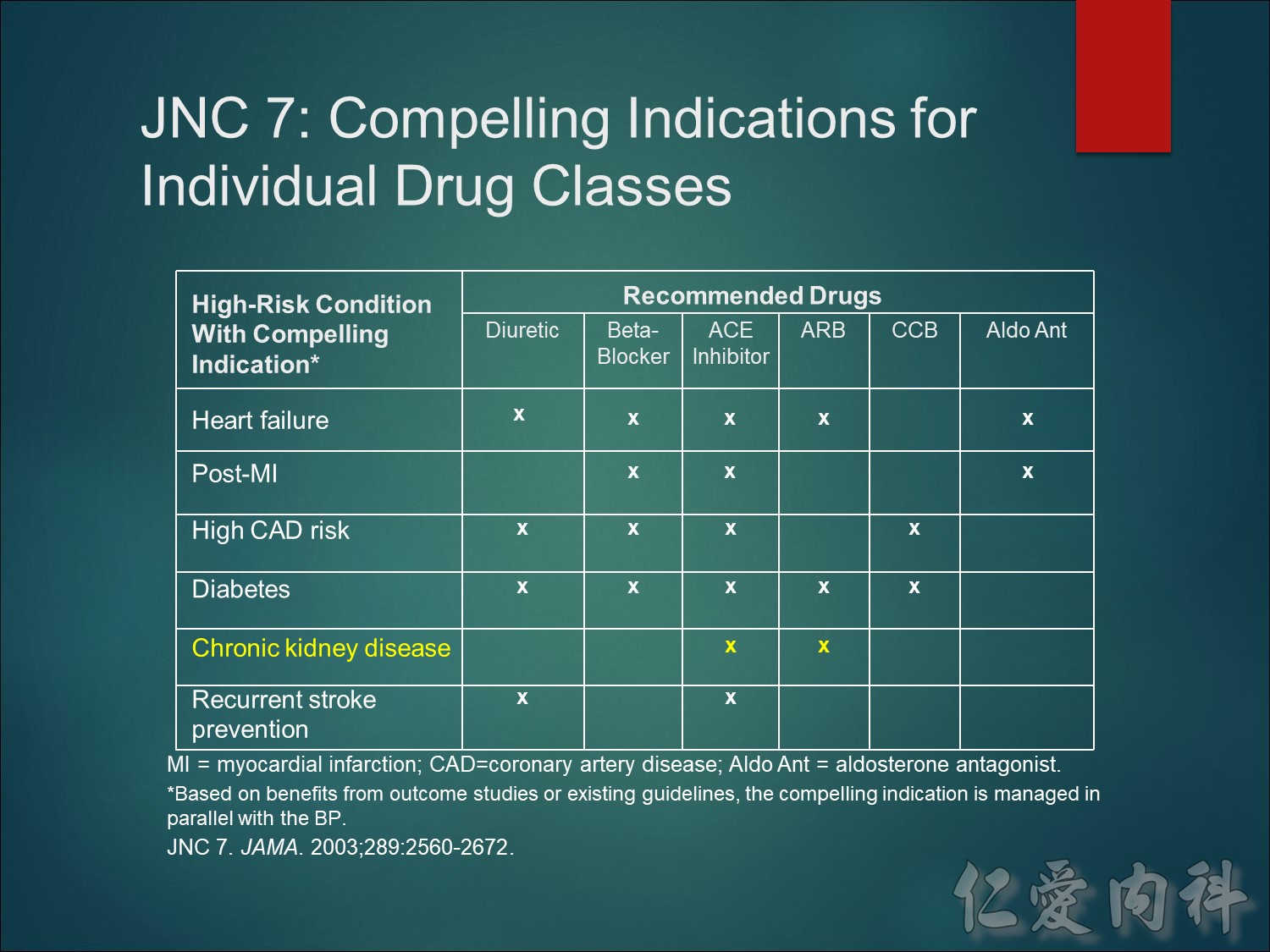
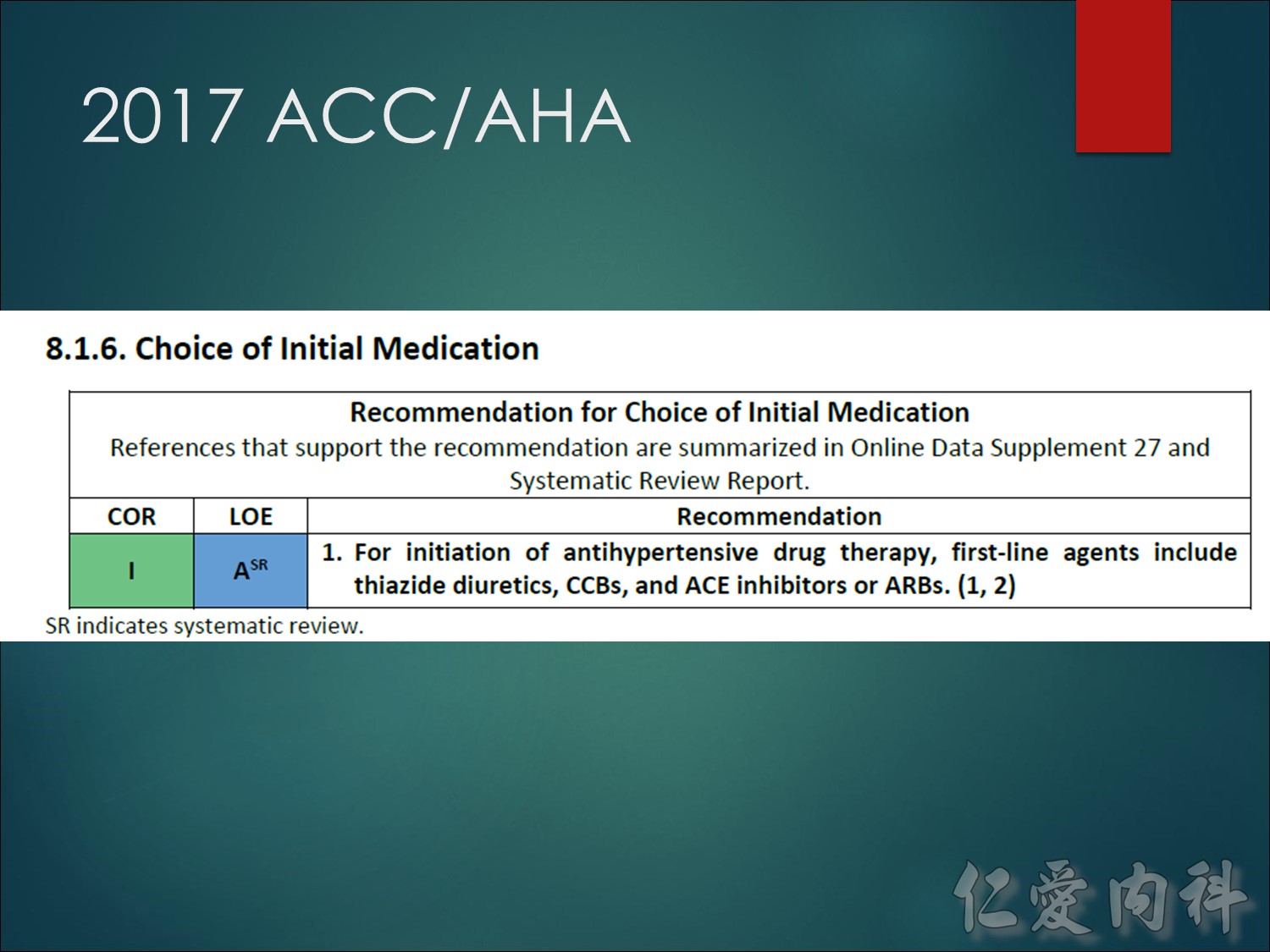
JNC 7 recommends thiazide diuretics, either alone or in combination with beta-blockers, ACE inhibitors, ARBs, or CCBs, as initial therapy for most patients.
ACE inhibitors and ARBs are recommended for patients with chronic renal disease.
Patients with recurrent stroke are best managed with a combination of thiazide diuretics and ACE inhibitors.
Patients with acute coronary syndromes should be treated initially with beta-blockers and ACE inhibitors.
CCBs are recommended in hypertensive patients with diabetes or with a high risk for coronary artery disease (CAD).
NOTES FOR PRESENTERS:
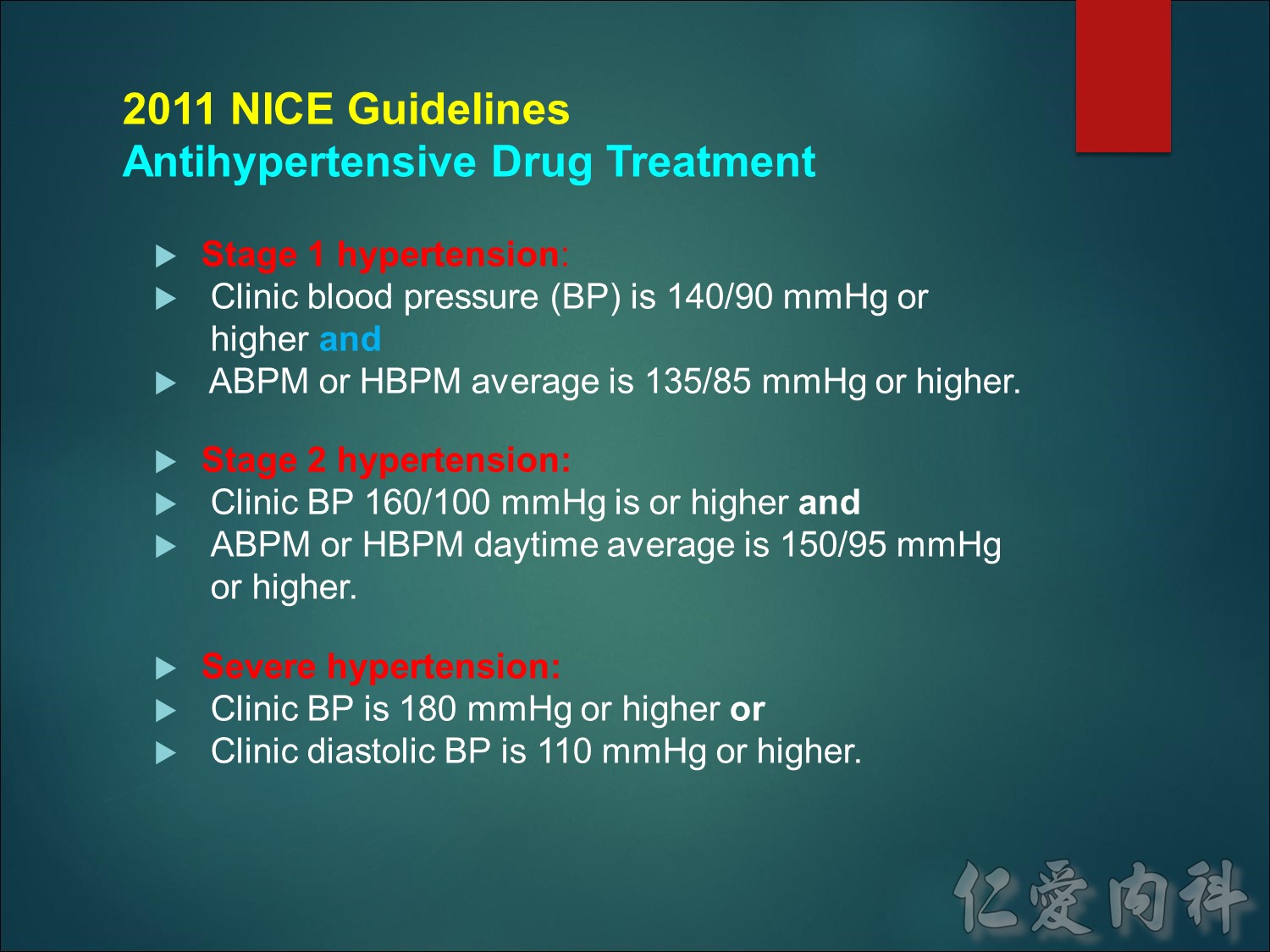
Definitions
In this guideline the following definitions are used:
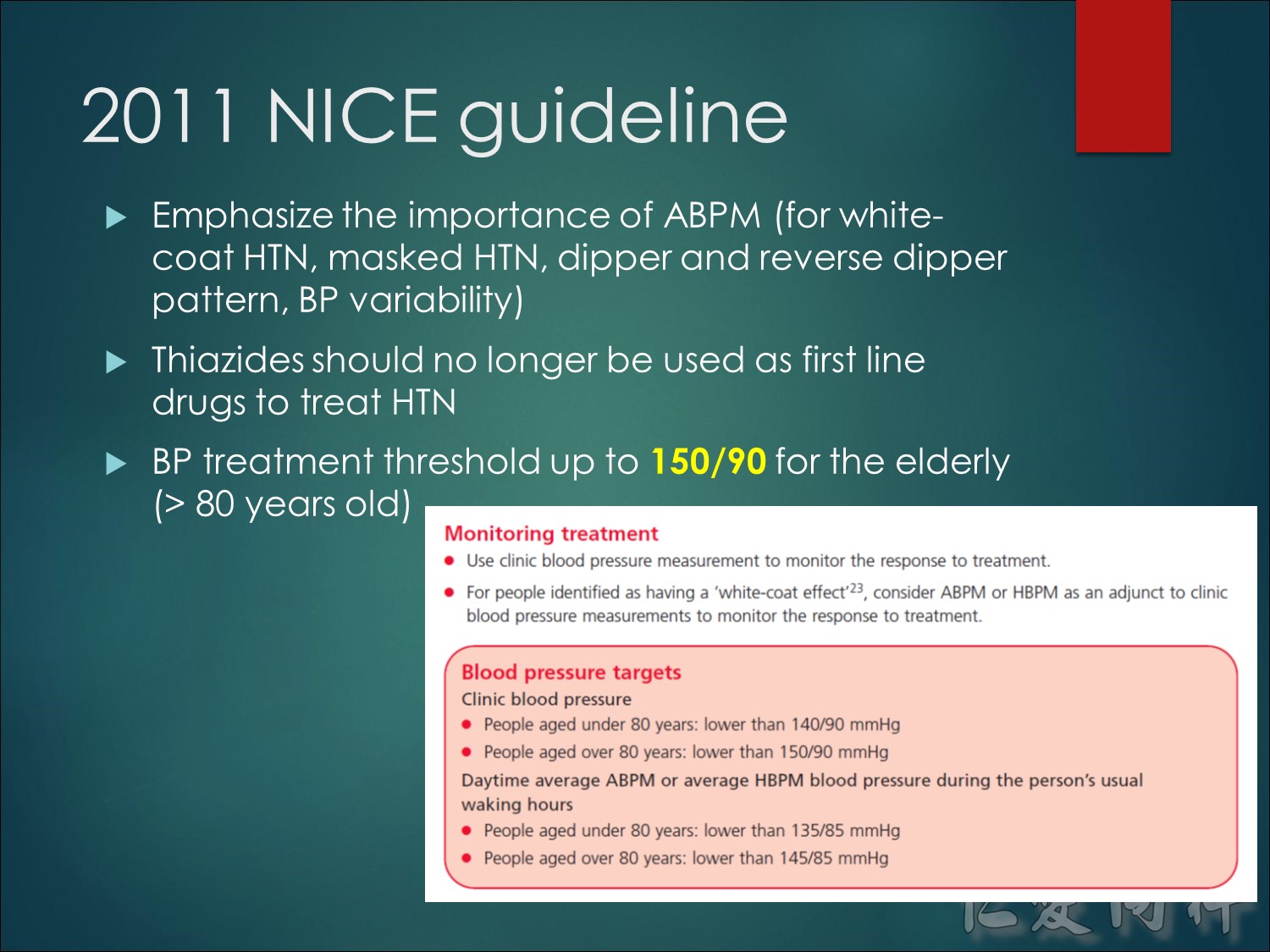
Stage 1 hypertension Clinic blood pressure is 140/90 mmHg or higher and subsequent ambulatory blood pressure monitoring (ABPM) daytime average or home blood pressure monitoring (HBPM) average blood pressure is 135/85 mmHg or higher.
Stage 2 hypertension Clinic blood pressure is 160/100 mmHg or higher and subsequent ABPM daytime average or HBPM average blood pressure is 150/95 mmHg or higher.
Severe hypertension Clinic systolic blood pressure is 180 mmHg or higher or clinic diastolic blood pressure is 110 mmHg or higher.
Additional information:
ABPM – ambulatory blood pressure monitoring
HBPM – home blood pressure monitoring

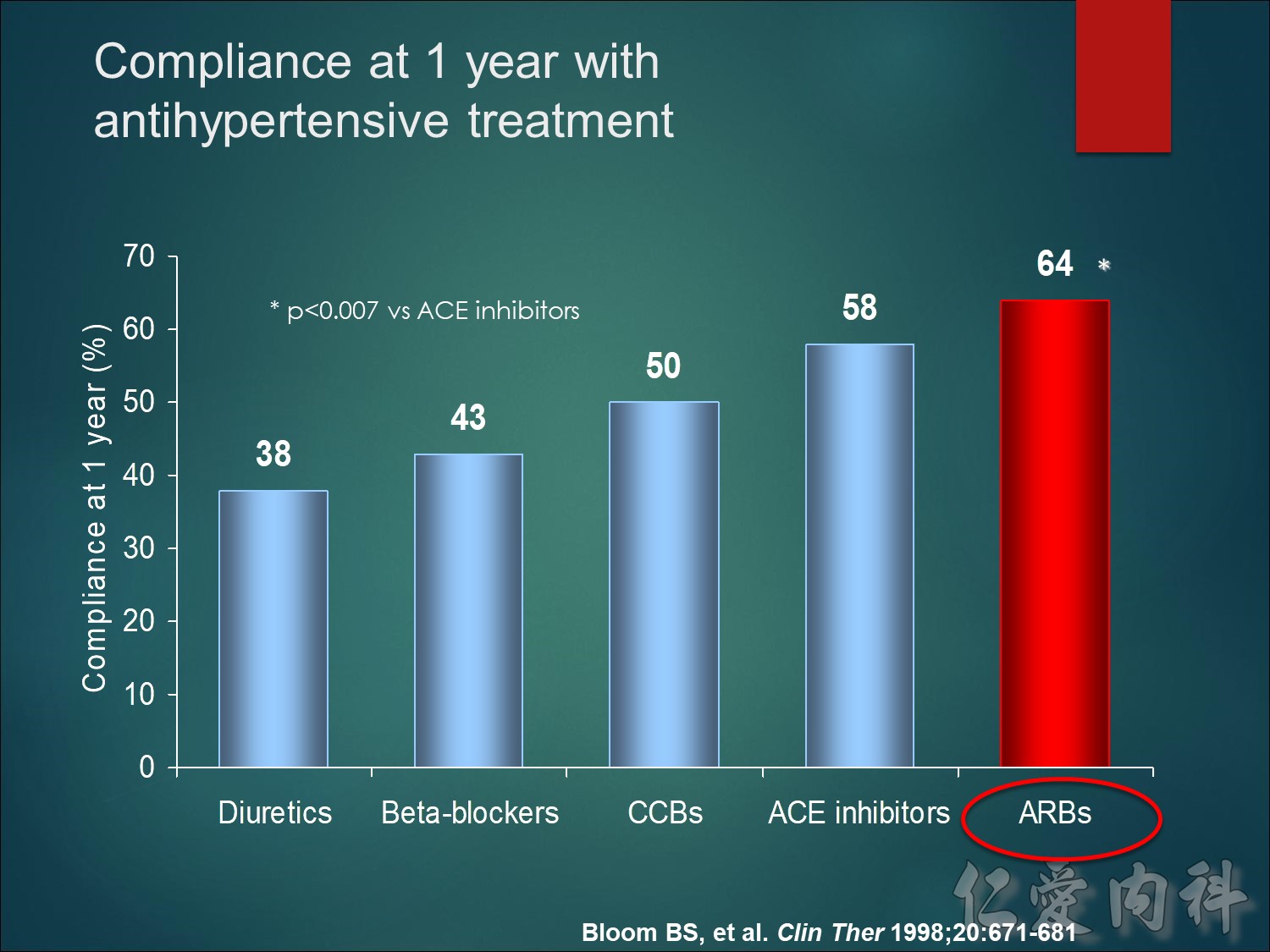
這張圖表說明不同類別降血壓藥物的服藥遵醫囑性差異。
儘管利尿劑經常做為高血壓病患的第一線療法,其遵醫囑性卻是最低的。β受體阻斷劑也沒好到哪裡去,而鈣離子通道阻斷劑(CCBs)和血管收縮素轉化酶(ACE)抑制劑的病患順從率則比較高。降血壓療法中,病患順從率最高的是血管收縮素II接受器阻斷劑(ARBs),因此醫生較常開立副作用緩和的降血壓藥物,如ARBs。
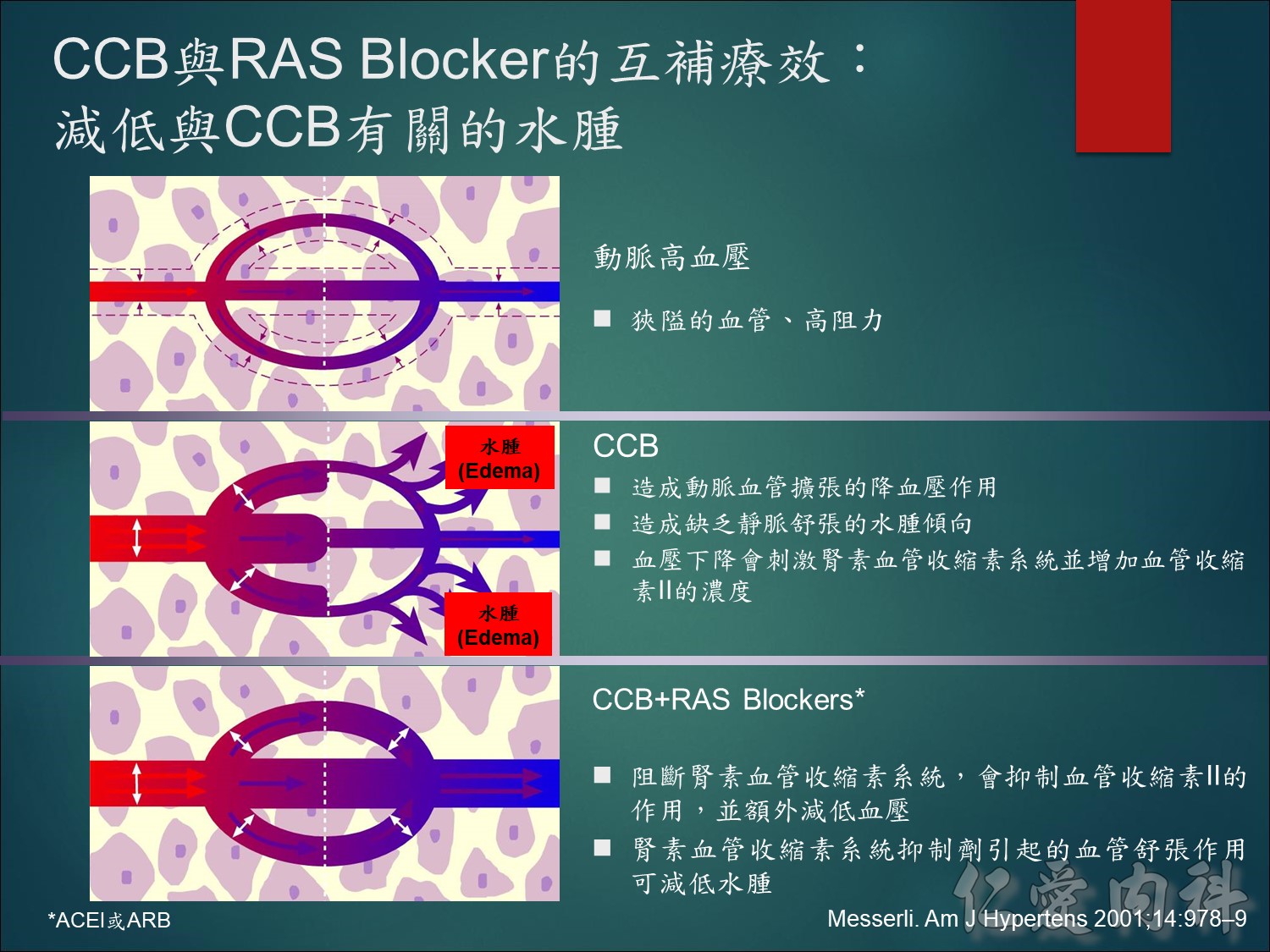
從這個意識圖我們可以看到一般的高血壓患者是動脈跟靜脈同時受到狹隘高阻力的狀態,那當我們單一投與一個CCB藥物的時候,CCB的作用只作用在動脈血管的內皮細胞,使動脈血管擴張達到降壓的效果,但由於高血壓是動靜脈同時的收縮,今天就像是高速公路的四線道,車流量非常的暢通,但忽然間前方道路的縮減,就像是我們動脈擴張靜脈沒有擴張的狀況下,血液的流量容易受到阻塞,滲透壓不平衡的狀態就容易造成腳踝水腫的狀況。所以如果我們能維持道路的暢通,就像我們的處方CCB時加上ARB的投與,同時擴張動靜脈的血管,可以緩解單用CCB所造成腳踝水腫的狀況。
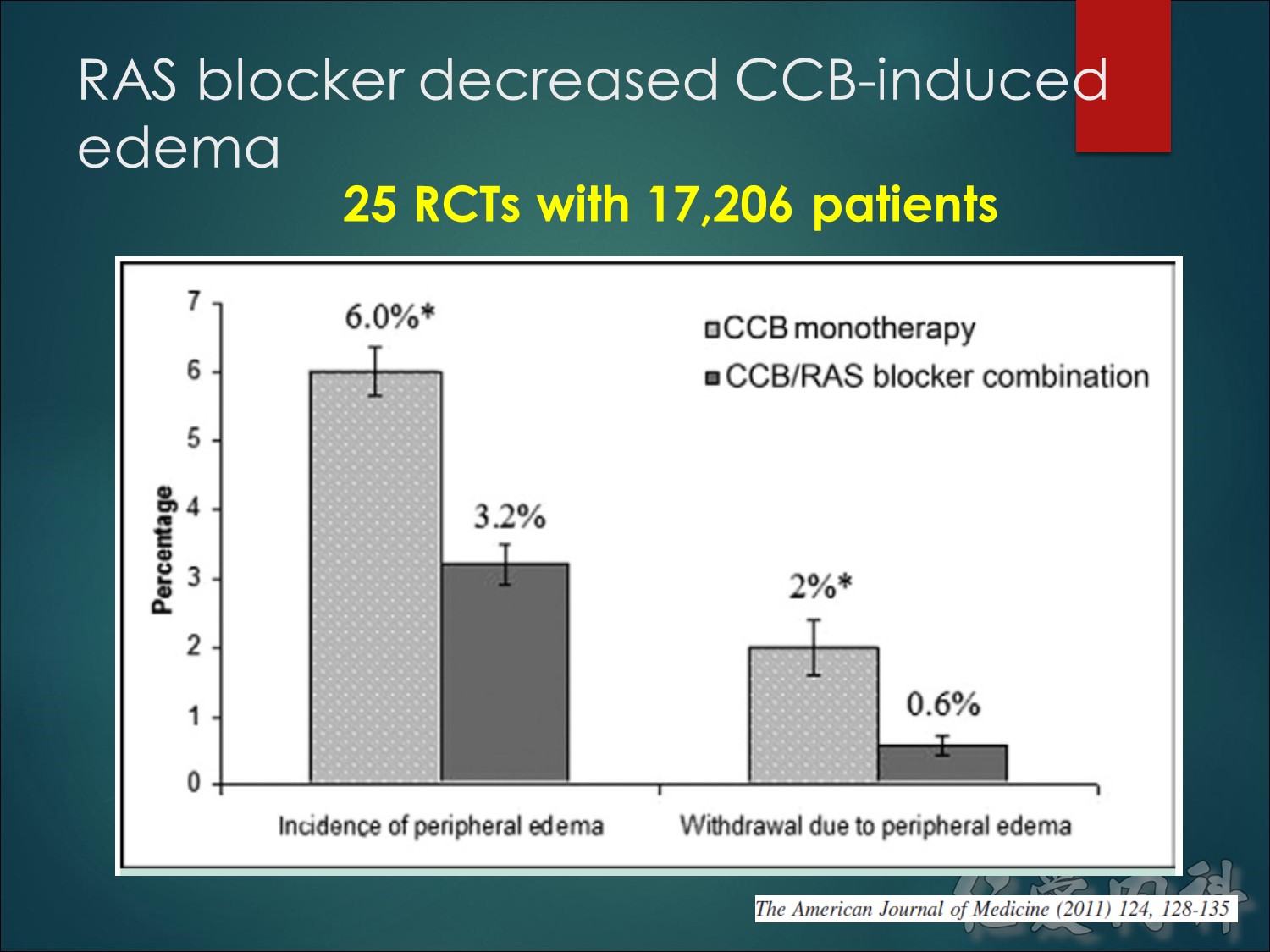
與鈣離子通道阻斷劑(CCB)有關的周邊水腫,乃因為動脈循環比靜脈循環具有較大之擴張作用,進而增加跨微血管壁的梯度與微血管滲漏所造成。
加入腎素血管收縮素系統(RAS)阻斷劑,有助於使此作用失效,因為RAS阻斷劑會使動脈和靜脈微血管床擴張,並將跨微血管壁的壓差回復至正常值。如此可減低CCB誘發水腫的可能性。
注意:
周邊性水腫與容積過多無關。
加入利尿劑無助於緩解CCB誘發的周邊性水腫。
參考文獻
Messerli FH. Vasodilatory edema: a common side effect of antihypertensive therapy. Am J Hypertens 2001;14:978–9.
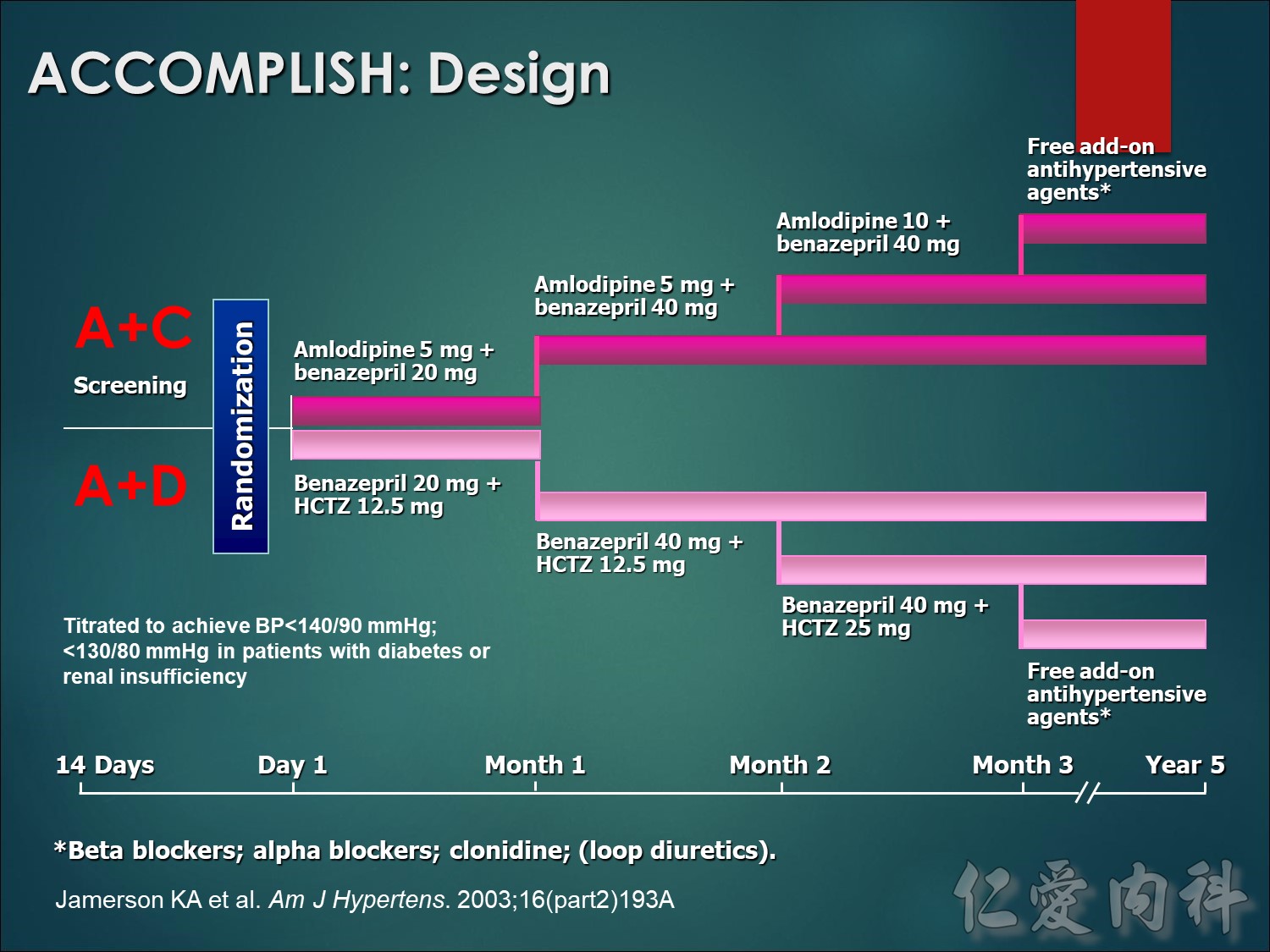
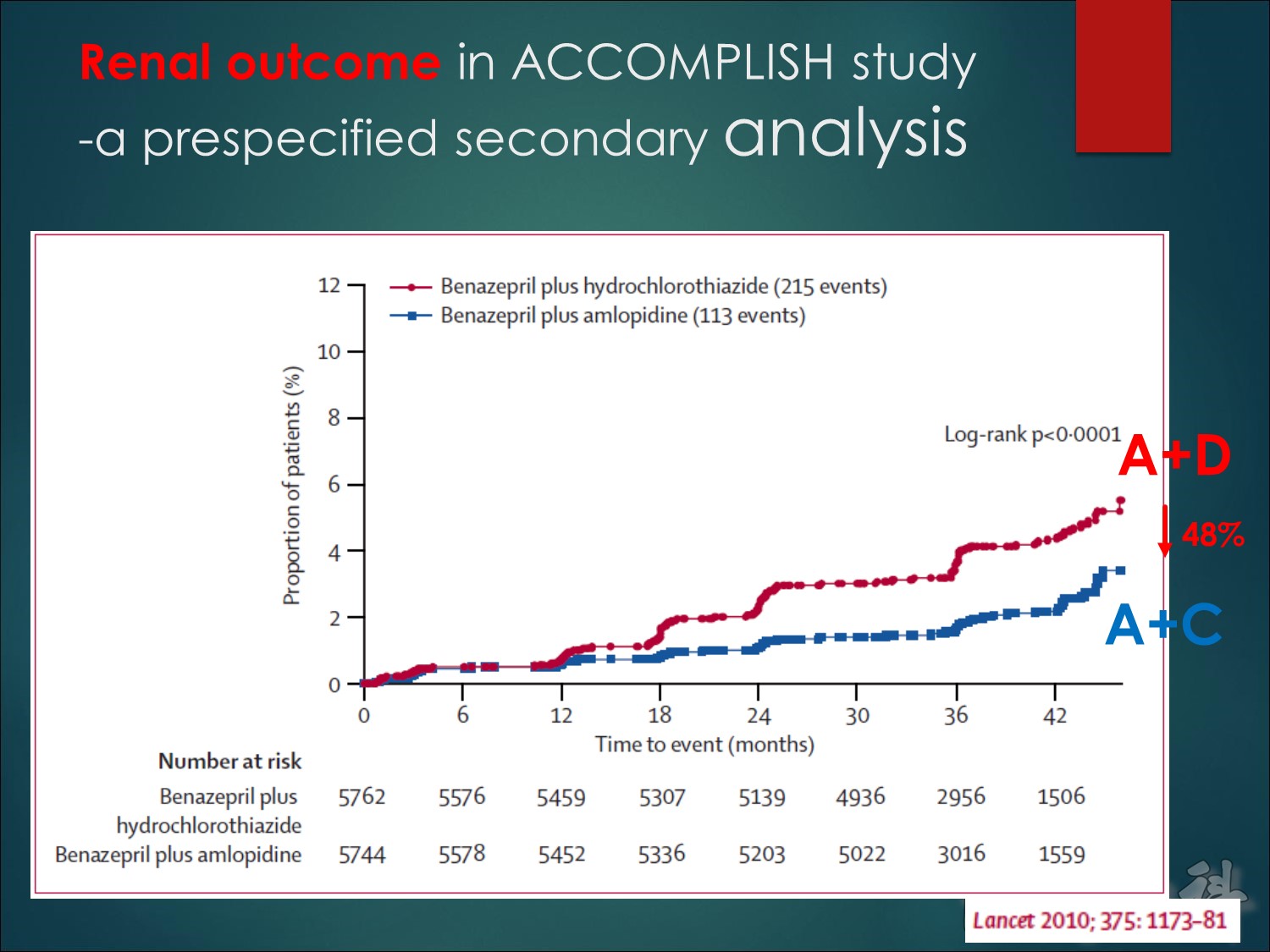
Patients will be randomized to amlodipine/benazepril 5/20 mg or benazepril/HCTZ 20/12.5 mg, and will have their doses force-titrated to standard maintenance doses of amlodipine/benazepril 5/40 mg, and benazepril/HCTZ 40/12.5 mg during the first 2 months. The doses can be increased to 10/40 mg or 40/25 mg, respectively, and after 3 months other antihypertensive agents (excluding the drug classes involved in the primary treatments) may be added to achieve blood pressure <140/90 mmHg (<130/80 mmHg for patients with diabetes or renal insufficiency). Investigators will be strongly encouraged to reach target blood pressure in all patients. Patients will be seen at 3 months, 6 months, and thereafter at 6-month intervals until the end of the trial.1 (Jamerson et al. Am J Hypertens. 2004;17: Page 796-A)
ACCOMPLISH is an event-driven trial: patients will be treated until 1,642 primary cardiovascular events have been reported. It is estimated this will take approximately 5 years, including the 18 months of recruitment.
- Jamerson KA, Bakris GL, Wun CC, et al. Rationale and design of the Avoiding Cardiovascular events through COMbination therapy in Patients LIving with Systolic Hypertension (ACCOMPLISH) trial: the first randomized controlled trial to compare the clinical outcome effects of first-line combination therapies in hypertension. Am J Hypertens. 2004;17:793–801.
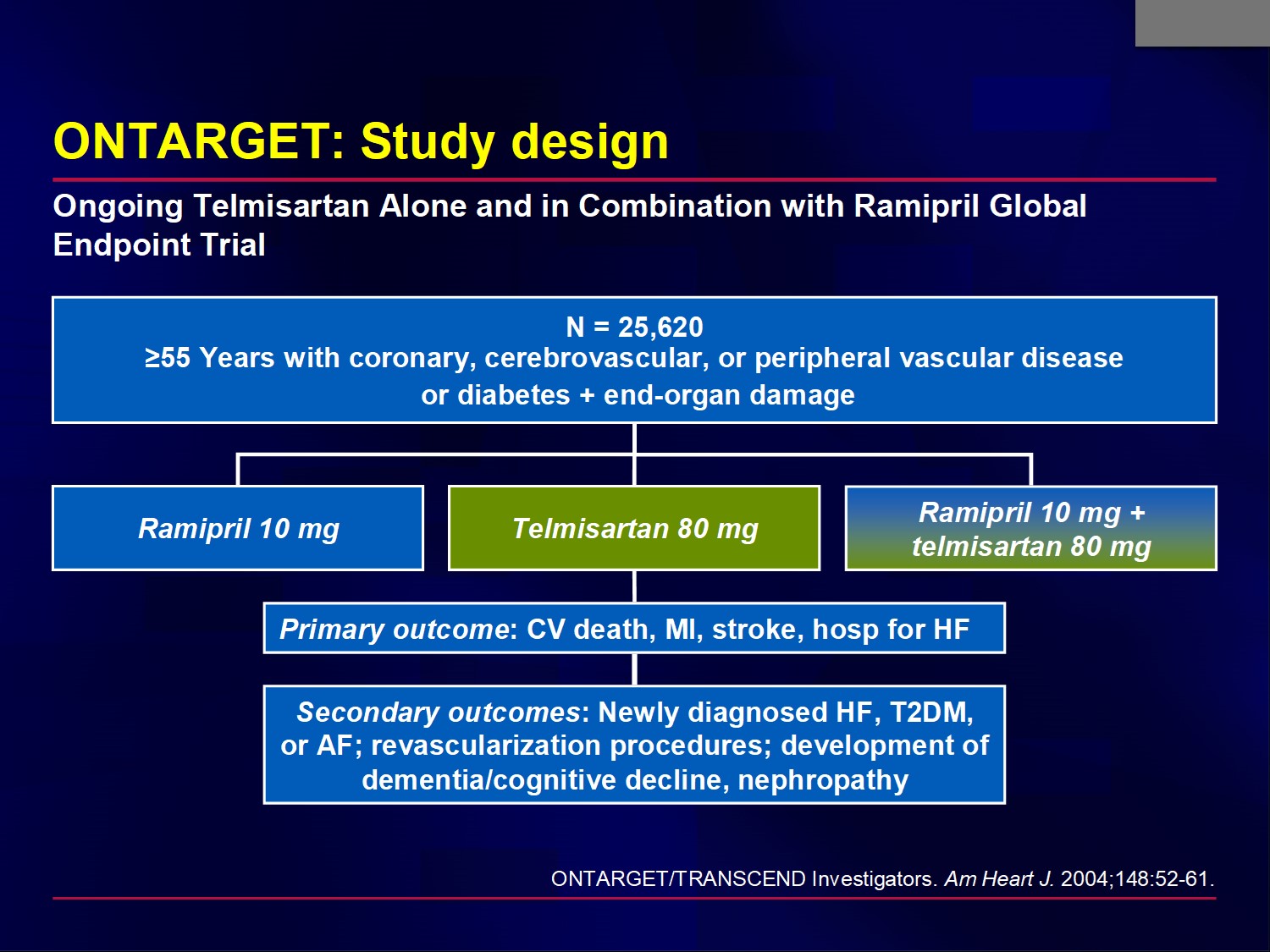
The ONTARGET study compared an ACEI vs an ARB vs a combination of both in high-risk individuals similar to those in the HOPE trial, ie, aged 55 years or older with a previous coronary artery, peripheral artery, or cerebrovascular event, or diabetes with evidence of target organ damage.
Patients with uncontrolled hypertension on treatment (ie, BP >160/100 mm Hg) or symptomatic HF were excluded.
The primary objectives of ONTARGET were to determine:
If the combination of telmisartan 80 mg daily and ramipril 10 mg daily is more effective in reducing the composite outcome than ramipril 10 mg alone.
Whether telmisartan 80 mg daily is at least as effective (ie, “not inferior”) as ramipril 10 mg daily as monotherapy.
The secondary objectives were development of newly diagnosed HF, T2DM, or atrial fibrillation; the need for revascularization procedures, development of dementia/cognitive decline, and nephropathy.
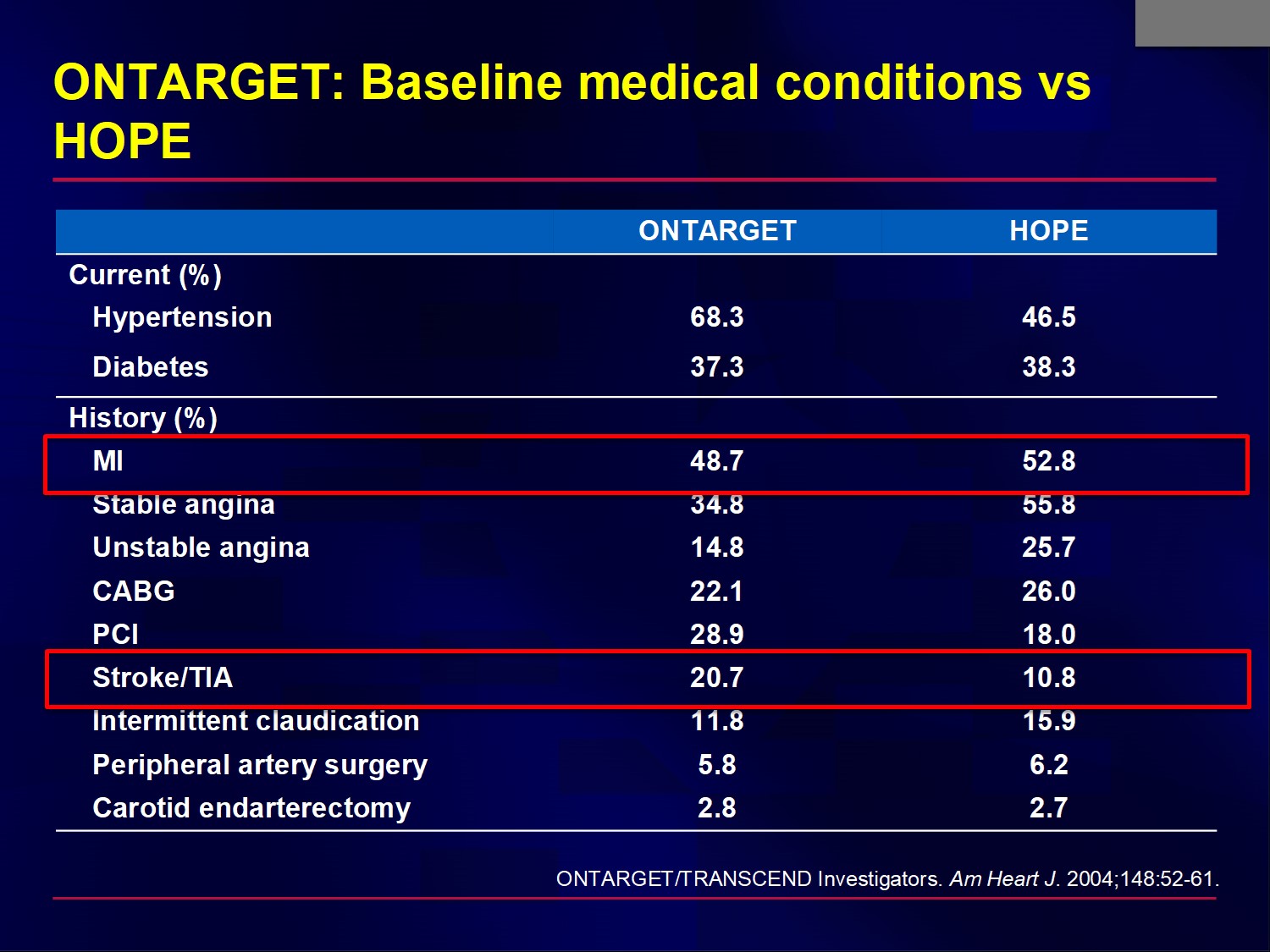
By design, the patients enrolled in ONTARGET were comparable to those in HOPE; ie, they were at high risk for a CV event.
A higher proportion of patients in ONTARGET had hypertension and cerebrovascular disease.
Abbreviation:
TIA = transient ischemic attack
Key point: Statistical adjustment for small differences in Blood Pressure in the treatment arms did not materially alter the results
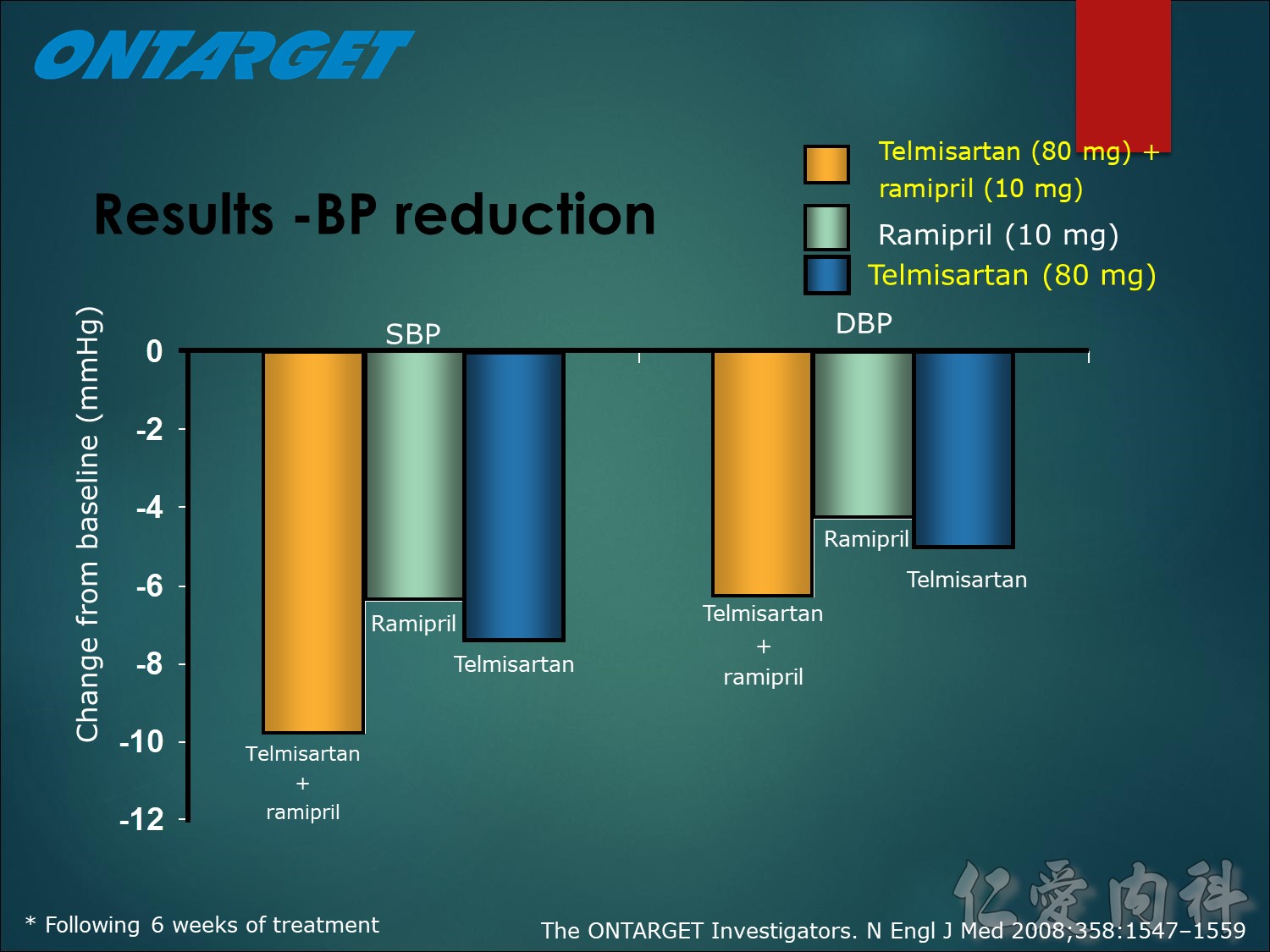
BP reduction
The quasi complete decrease in mean BP was achieved afetr 6 weeks of run-in treatment, with respective decreases for telmisartan alone (reduction of), ramipril alone and their combination combination of 7.4/5.0mmHg , 6.4/4.3 mmHg and 9.8/6.3 mmHg respectively. Throughout the course of the study, patients in both telmisartan groups demonstrated relatively lower BP levels (mean reductions of 0.9/0.6 mmHg and 2.4/1.4 mmHg, respectively) versus ramipril alone.
However, adjustment for the small differences in BP did not materially alter the results for primary outcome (relative risk for telmisartan vs ramipril 1.02, 95% CI; 0.95 to 1.10, relative risk for the combination vs ramipril 1.00, 95% CI; 0.93 to 1.10)
References
- The ONTARGET Investigators. Telmisartan, ramipril, or both in patients at high risk for vascular events. N Engl J Med 2008;358:1547–1559.
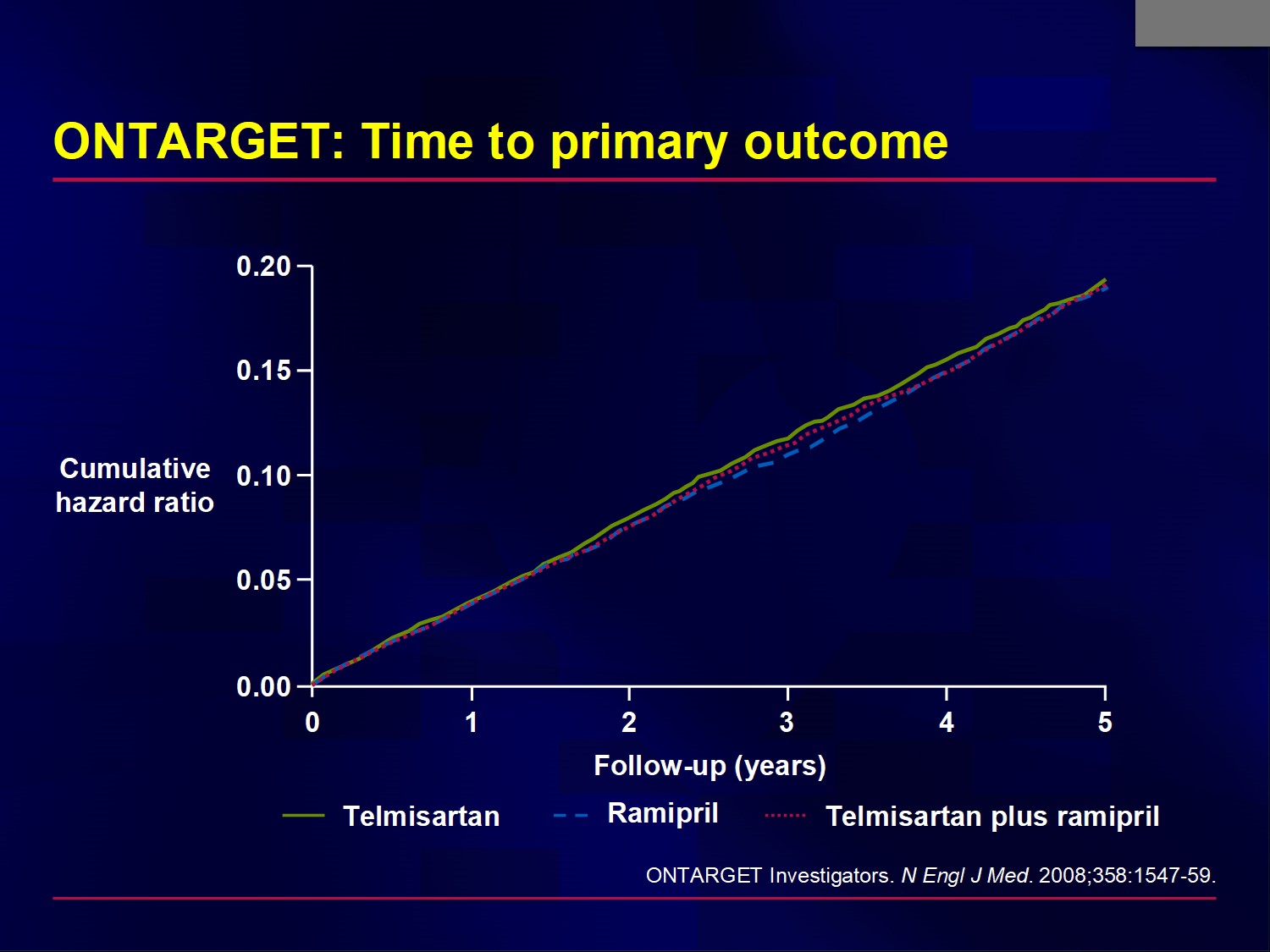
The primary outcome occurred in 16.5%, 16.7%, and 16.3% of patients in the ramipril, telmisartan, and combination groups, respectively.
Hazard ratio for telmisartan vs ramipril 1.01, 95% CI 0.94-1.09
Hazard ratio for combination vs ramipril 0.99, 95% CI 0.92-1.07
AT1-receptor binding affinity― Potent receptor blockade
AT 1 affinity The specific AT1 affinity relates to how specificially attracted the medicine is for the correct receptor.
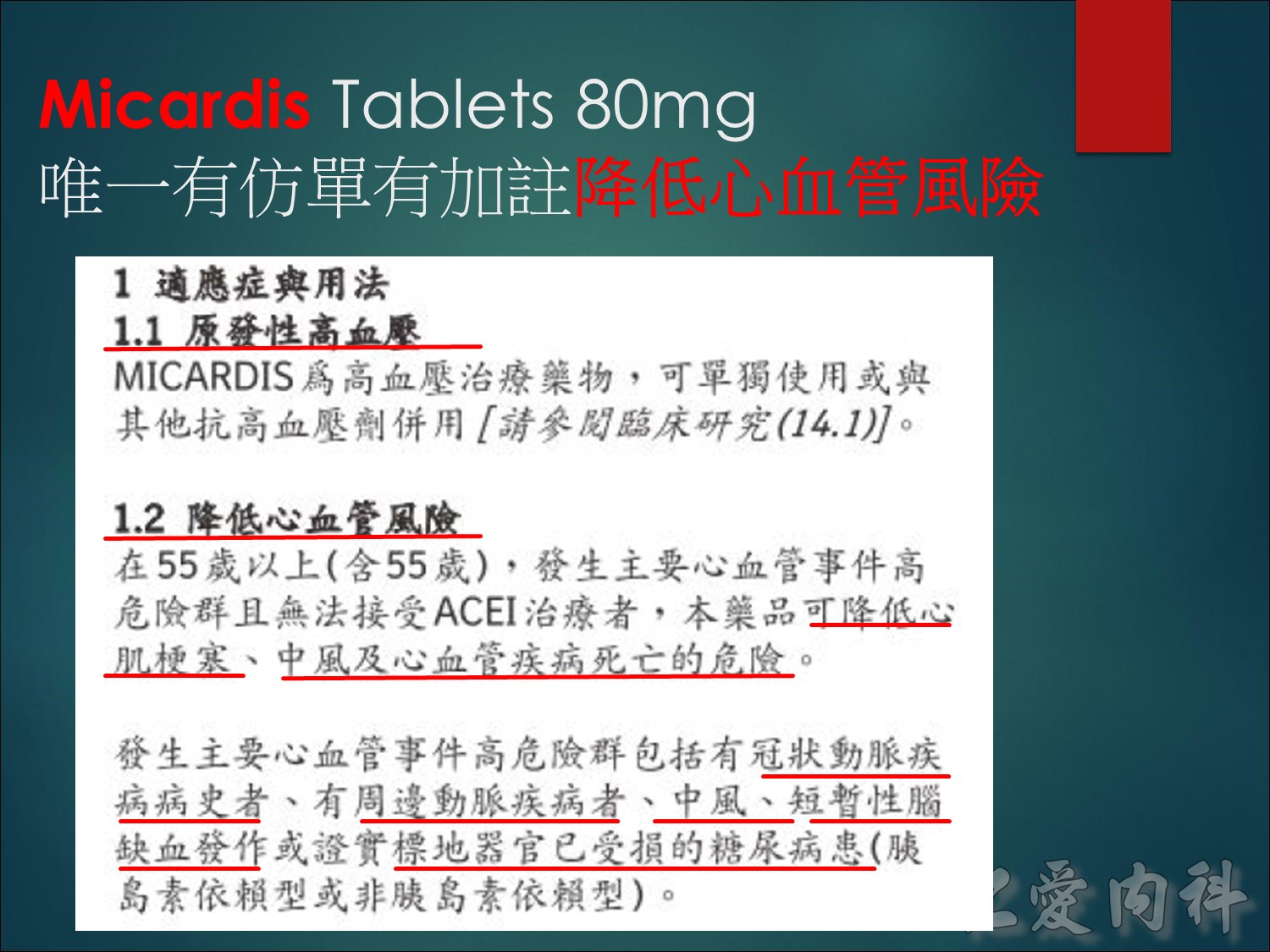
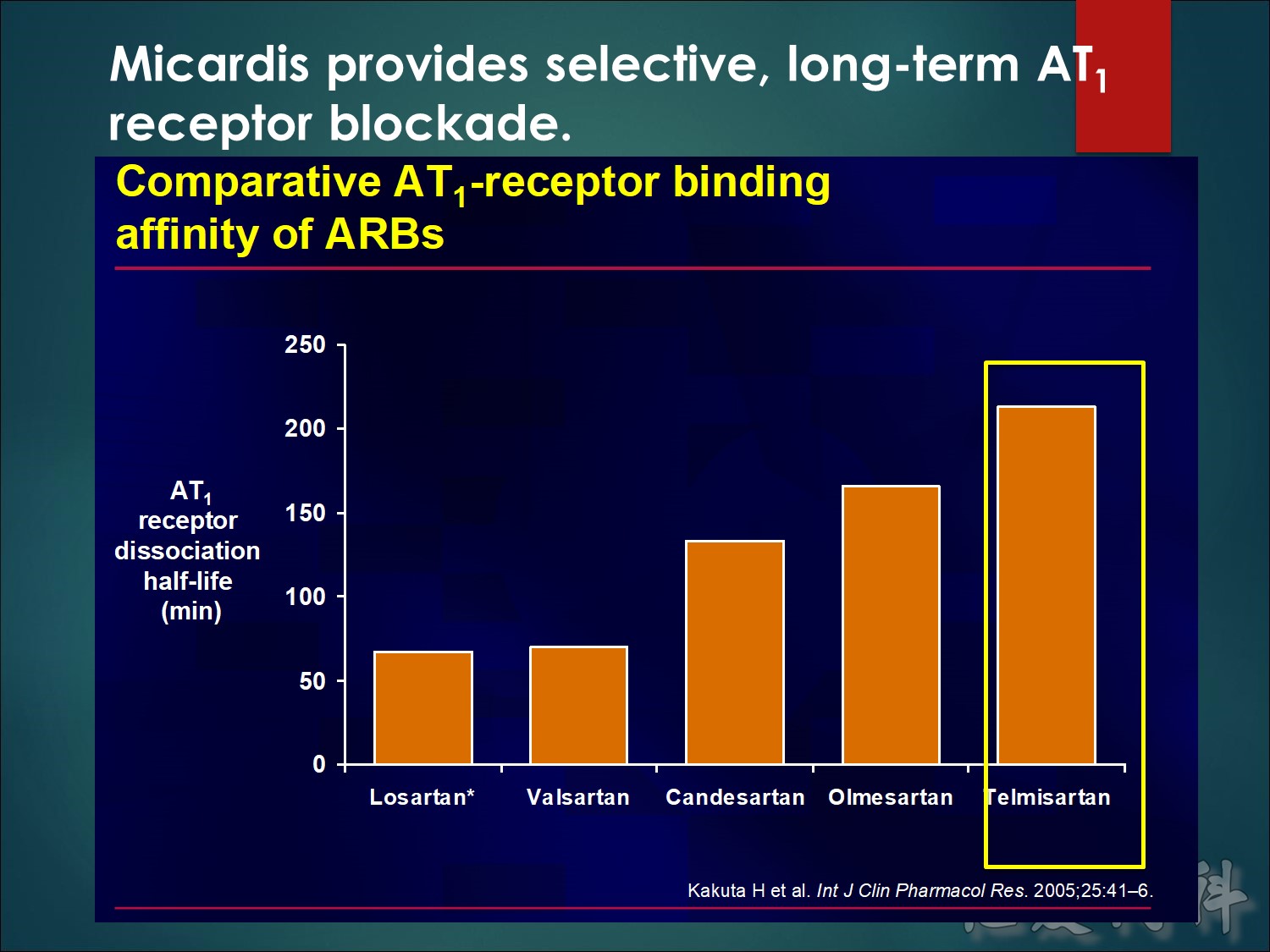
Telmisartan provides selective, long-term AT1 receptor blockade.
In this in vitro study of membrane-bound, human angiotensin II type 1 (AT1) receptor, the rank order of binding affinity was telmisartan > olmesartan > candesartan ³ valsartan ³ losartan.1
The respective dissociation rate constants were 0.0032, 0.0042, 0.0052, 0.0099 and 0.010 min–1.
These results demonstrate that telmisartan has the strongest binding affinity to AT1 receptor among various ARBs tested. The rank order of affinity was telmisartan > olmesartan > candesartan > EXP3174 > or = valsartan > or = losartan. The present findings suggest that telmisartan (Micardis) may have long-lasting blood pressure-lowering effects and superior cardiovascular-protective properties in patients with hypertension due to its strongest AT1 receptor antagonistic ability.
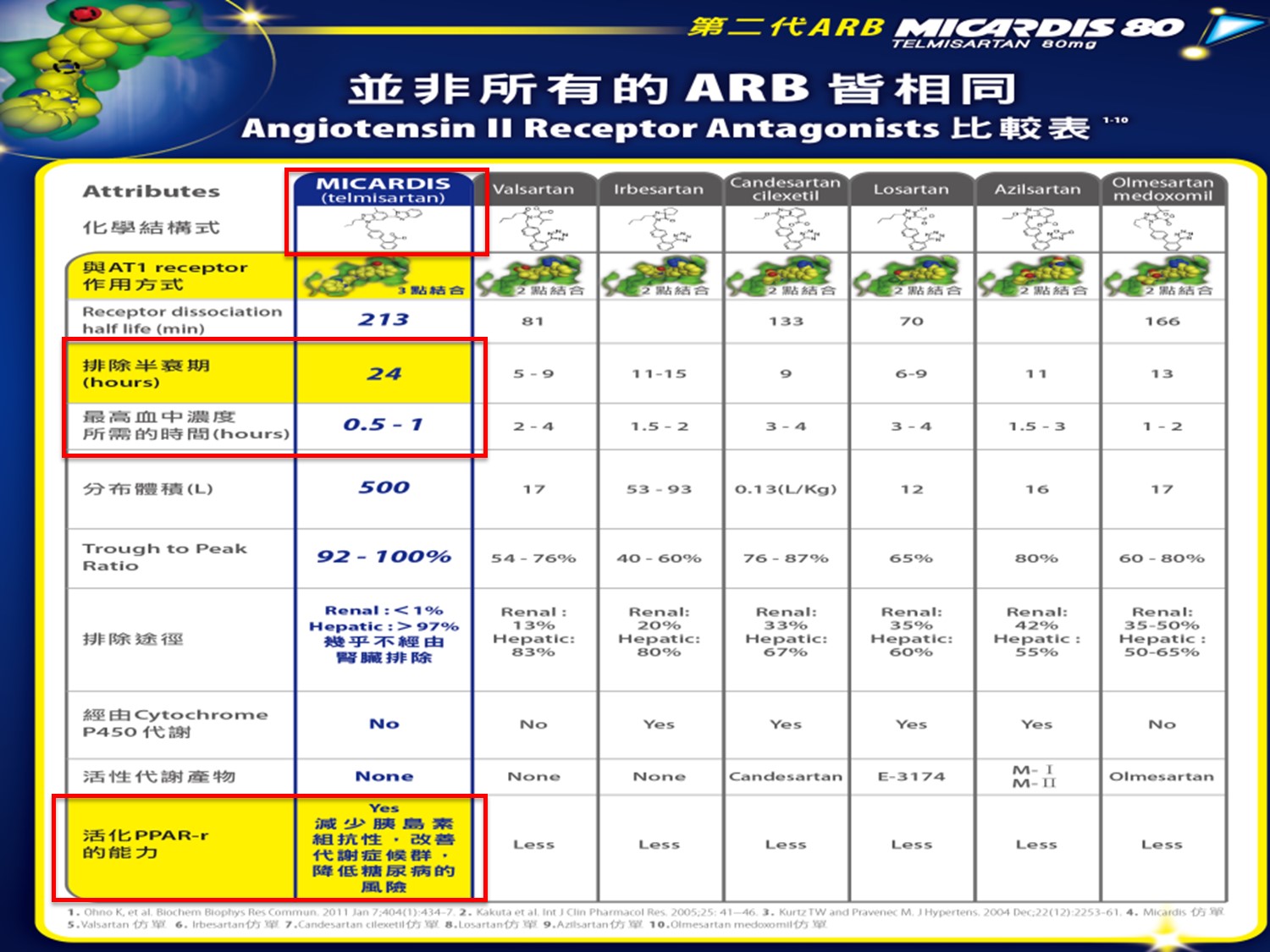
The respective dissociation half-lives were 213, 166, 133, 70 and 81 min.
In a separate study, telmisartan displaced 125I-AII from the AT1 receptor binding sites in rat lung preparations, with an inhibitor constant (Ki) of 3.7 nM.2 In this model, the Ki for losartan was 24 nM, which is about a sixth of the potency of telmisartan.
Additionally, telmisartan displays no affinity for the AT2 receptor (Ki >10,000 nM) or for acetylcholine, adenosine, catecholamine, dopamine, histamine, serotonin or imipramine receptors.
References
Kakuta H., et al. Telmisartan has the strongest binding affinity to angiotensin II type 1 receptor: comparison with other angiotensin II type 1 receptor blockers. Int J Clin Pharmacol Res 2005;25:41–46
Wienen W. et al. Pharmacological characterization of the novel nonpeptide angiotensin II receptor antagonist, BIBR 277. Br J Pharmacol 1993;110:245–252
Long plasma half-life ― 24-hour efficacy
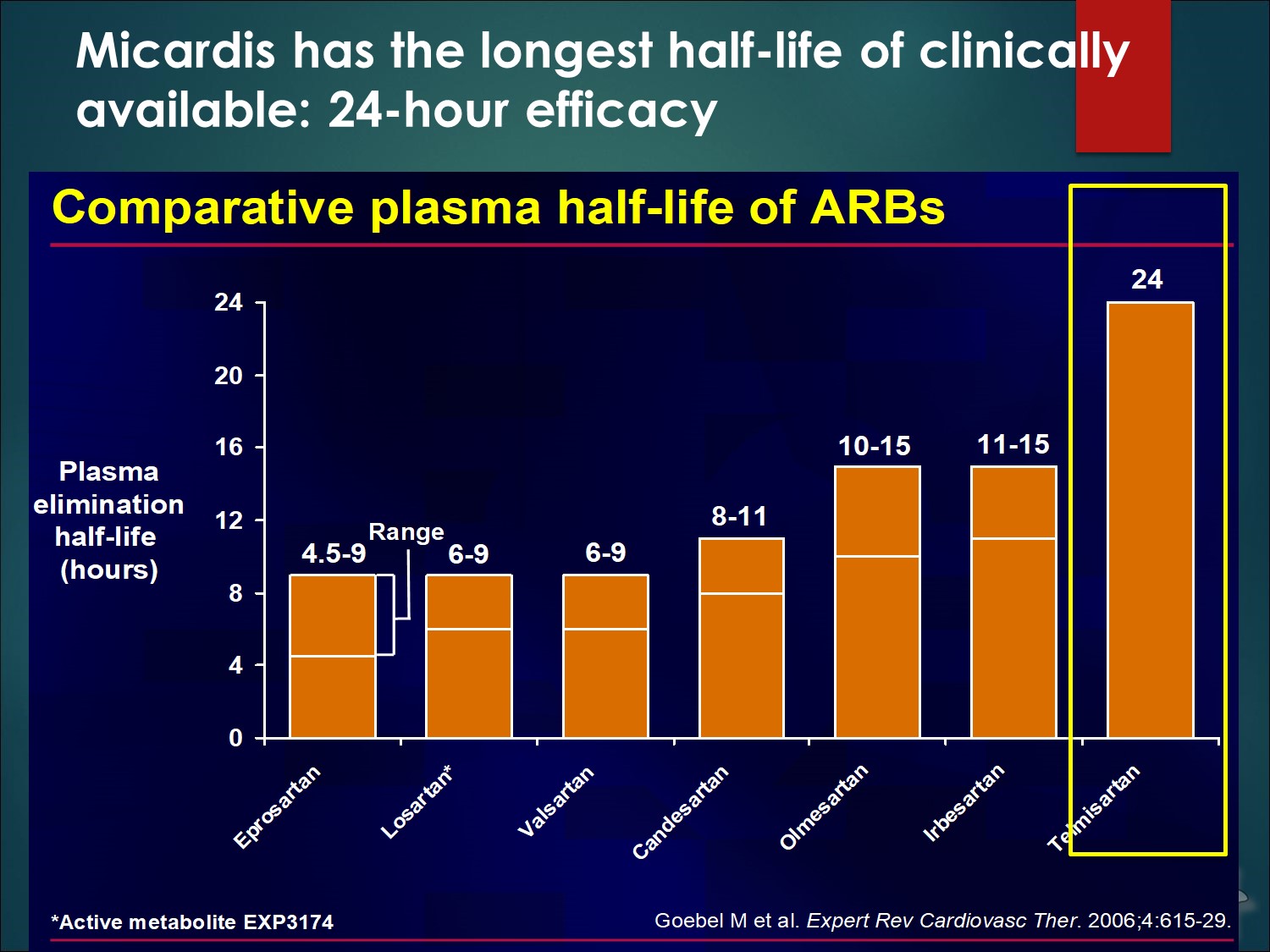
Telmisartan has a 24-h plasma half-life, which is the longest of any ARB.1,2
Telmisartan has the longest duration of action, with a terminal elimination half-life of around 24 h in comparison with 11–15 h for irbesartan, the ARB with the next longest half-life. The long duration of action and insurmountable binding to the receptor may be related to the slow dissociation kinetics of the antagonists from the AT1 receptor. Comparative clinical studies suggest that, at the recommended dose, losartan, the original drug in this class, has a lower antihypertensive efficacy than the newer agents, such as telmisartan. It is possible that these differences between angiotensin II receptor antagonists are due to variations in the degree and duration of receptor blockade, and may be of clinical significance with regard to the cardioprotective and renoprotective effects of this class of antihypertensive agents.
The long plasma half-life of telmisartan may be related to its efficacy as high plasma levels are maintained for the full 24-h dosing interval, including into the early morning hours.
References
- Burnier M. & Brunner H.R., Angiotensin II receptor antagonists.
Lancet 2000;355:637–645 - Brunner H.R., The new oral angiotensin II antagonist olmesartan medoxomil:
a concise overview. J Hum Hypertens 2002;16(Suppl 2):S13–S16
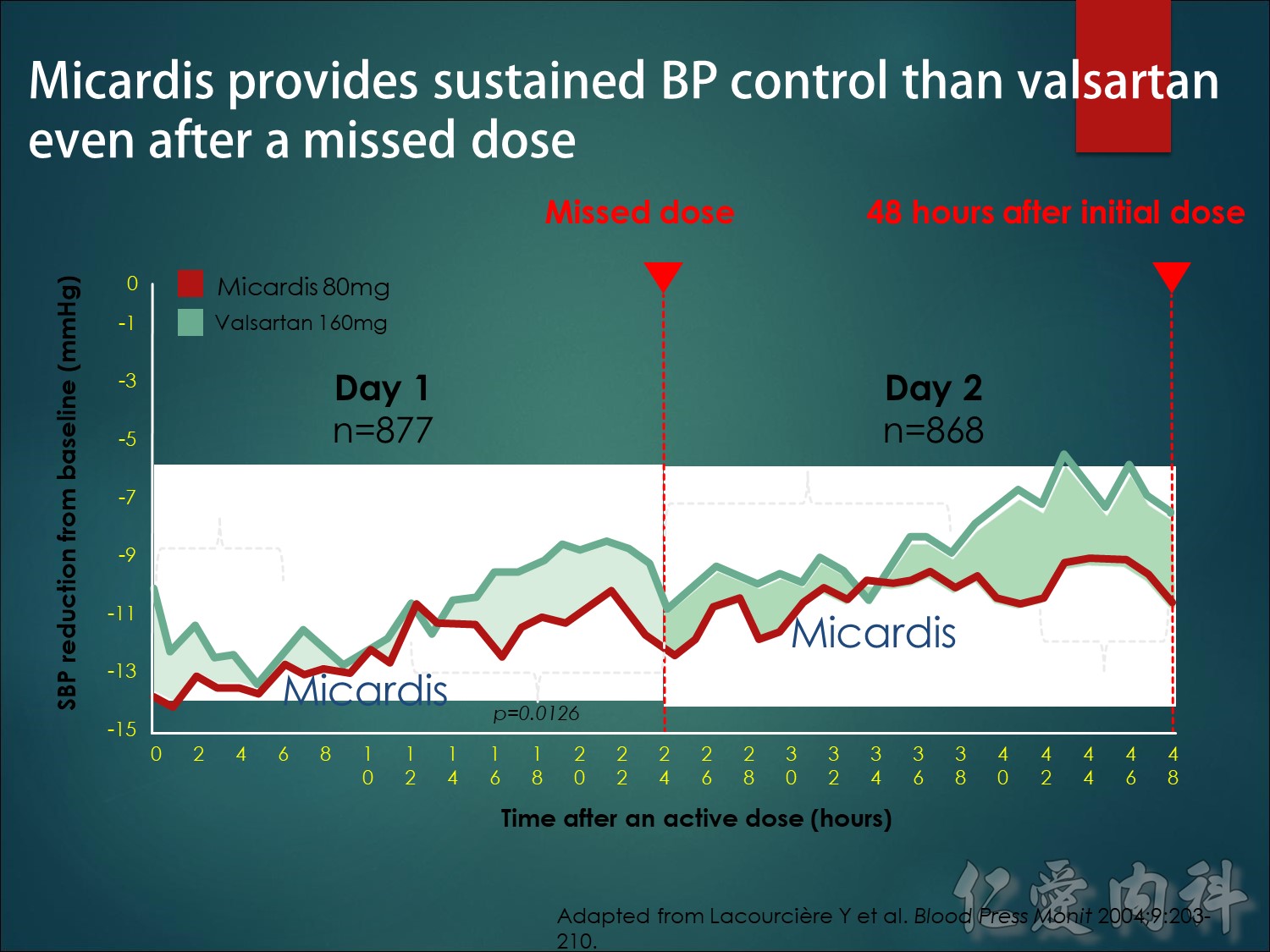
Telmisartan has the longest half-life of clinically available ARBs Telmisartan, with a terminal 24-hour half-life, may be the most effective ARB in controlling early morning surge in BP.
Telmisartan has the longest half-life of clinically available ARBs Telmisartan, with a terminal 24-hour half-life, may be the most effective ARB in controlling early morning surge in BP.
Micardis長達24小時的半衰期顯示出比其他ARB有更優異的降血壓作用 , 並且能防止清晨血壓的升高,在清晨時刻的血壓保護作用
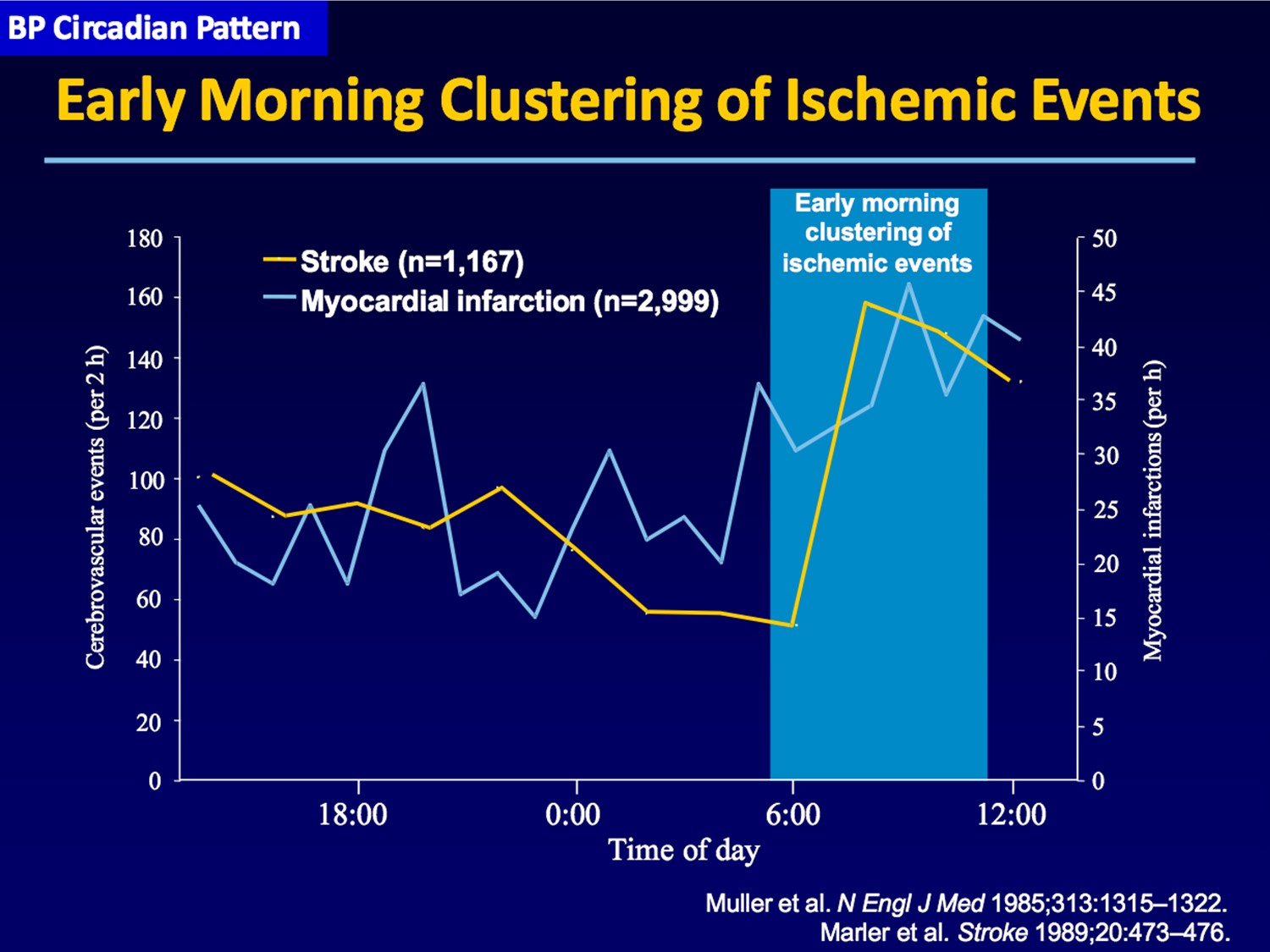
動態血壓監測顯示 通常睡眠期間血壓會下降10%~20%,並在清晨相當快速地增加,這清晨血壓上升顯示失去高血壓控制並且增加心肌的梗塞和中風的比例。
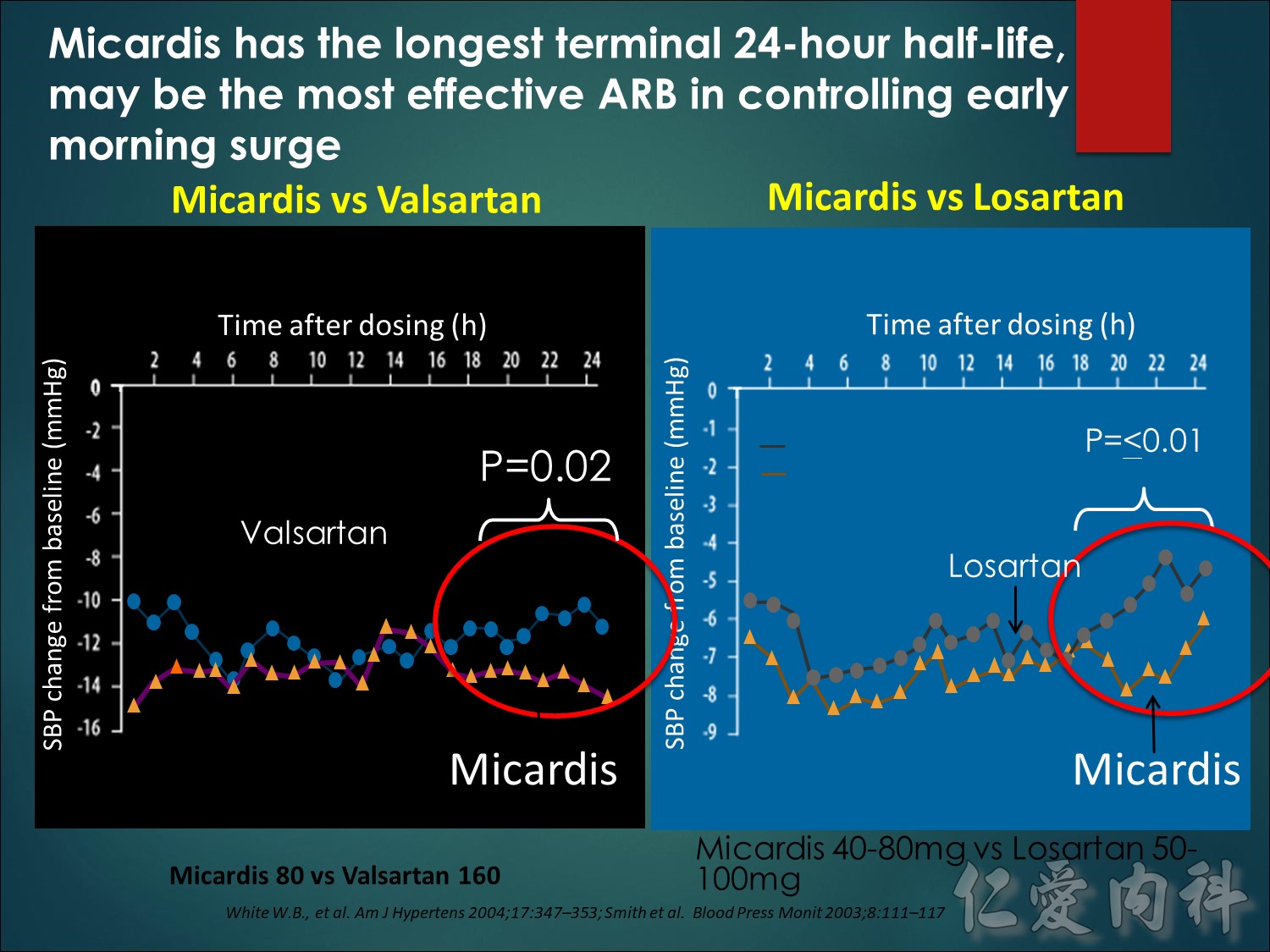
在這圖中顯示的兩項研究 , 可看出Micardis長達24小時的半衰期可能是臨床血壓控制的最重要的重點。懷特和他的同事在左側這項研究中,在控制血壓在24小時給藥期間的最後6個小時,Micardis被證明優於Valsartan。由史密斯右側的研究發現了與Losartan比較時也有類似的結果。
Telmisartan 24 h half-life translates into superior BP reductions versus other ARBs – BP protection during the early morning hours
Ambulatory blood pressure (BP) monitoring has shown that BP typically declines by 10% to 20% during sleep and increases fairly rapidly in the early morning period. This early morning rise in BP is associated with both loss of hypertension control and increased rates of myocardial infarction and stroke.
The two studies shown in this slide looked to see if the long 24-hour half-life of telmisartan could be clinically important at this critical point of BP control. In the study on the left, by White and colleagues, telmisartan was shown to be superior to valsartan, in controlling BP in the last 6 h of the 24-hour dosing period. The study on the right by Smith found a similar result when comparing telmisartan with losartan.
References
White W.B., et al. Effects of the angiotensin II receptor blockers telmisartan versus valsartan on the circadian variation of blood pressure: impact on the early morning period. Am J Hypertens 2004;17:347–353.
Smith D.H., et al. Comparison of telmisartan versus losartan: meta-analysis of titration-to-response studies Blood Press Monit 2003;8:111–117.
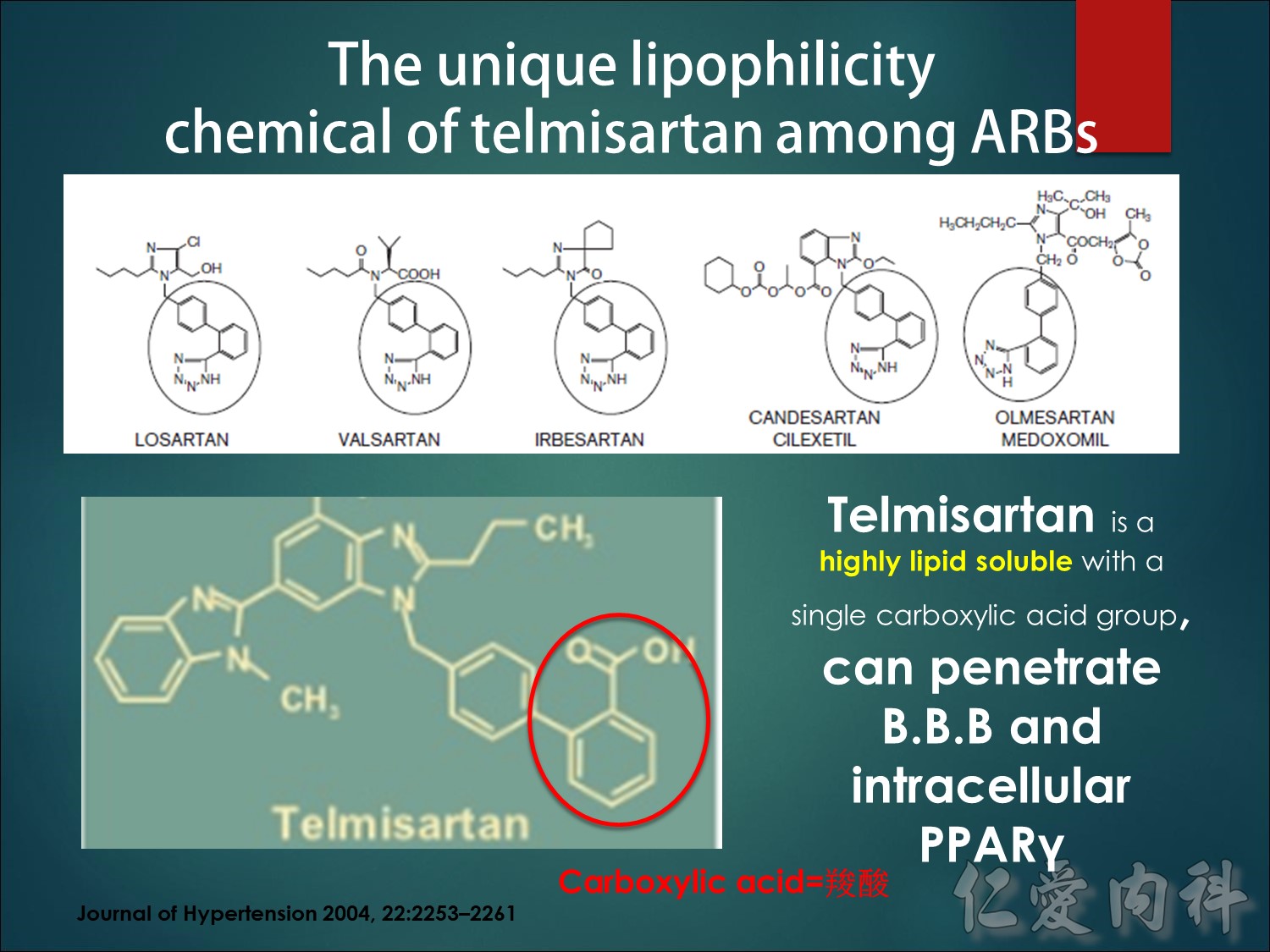
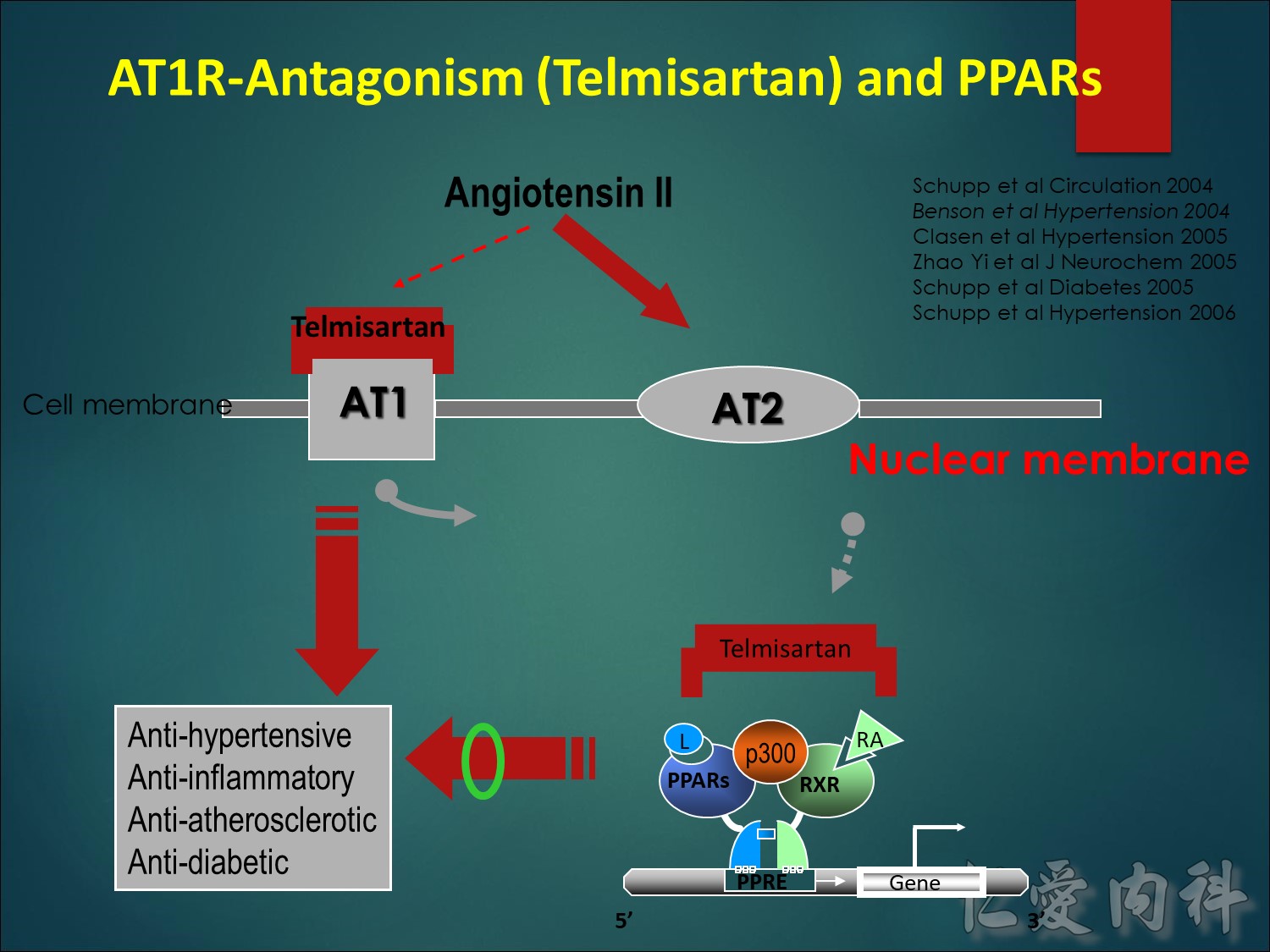
Telmisartan具備活化PPARγ的特色,與它獨特的化學結構式有關。Telmisartan 並沒有ARB所共有的 the biphenyl tetrazole 結構(圈選部分) ,只是簡單的carboxylic acid結構,而提高Telmisartan的脂溶性。
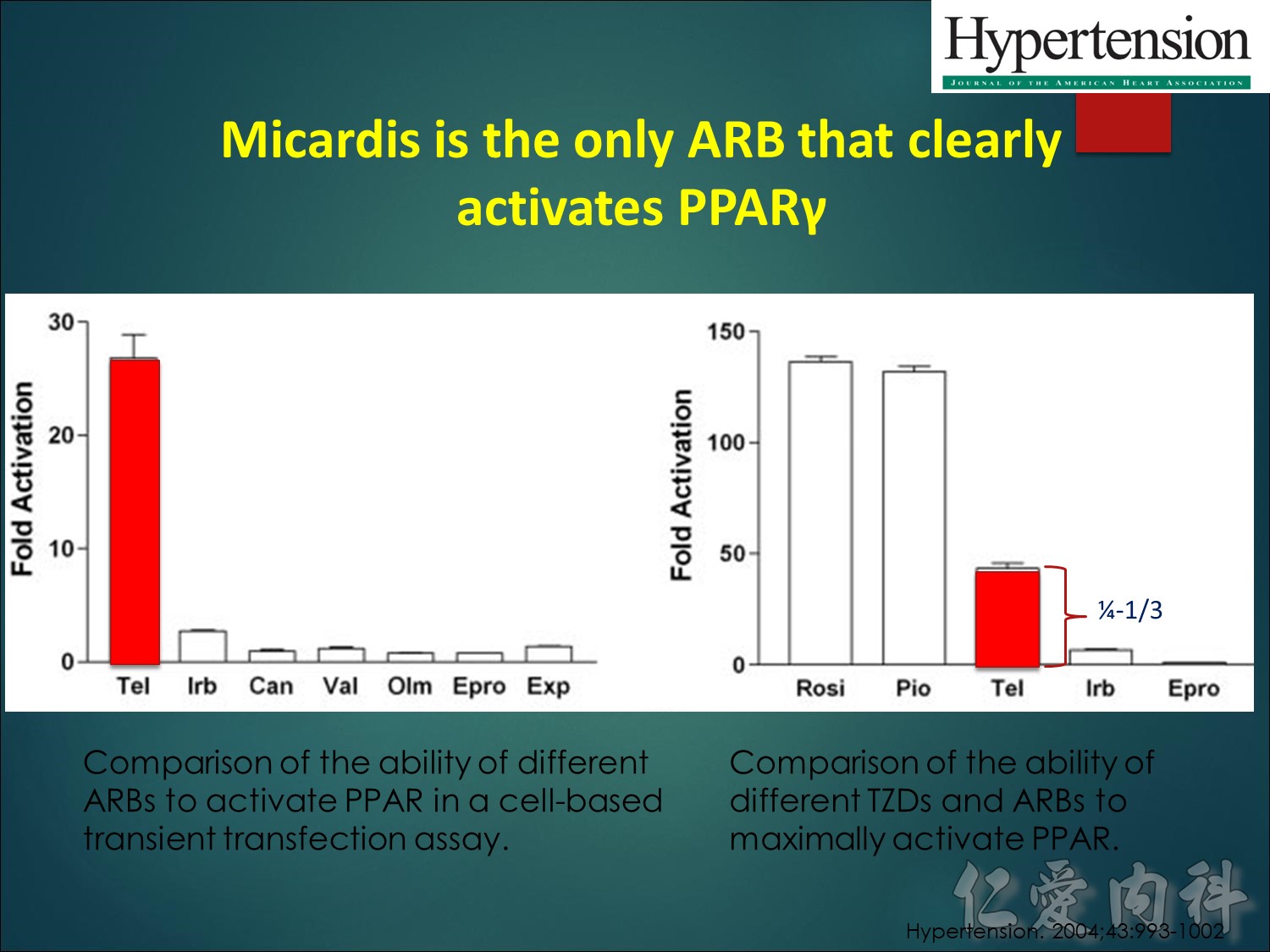
除了ARB,Telmisartan活化PPARγ的效力也與TZD做一比較,證實Telmisartan具有相當的PPARγ活化效力。
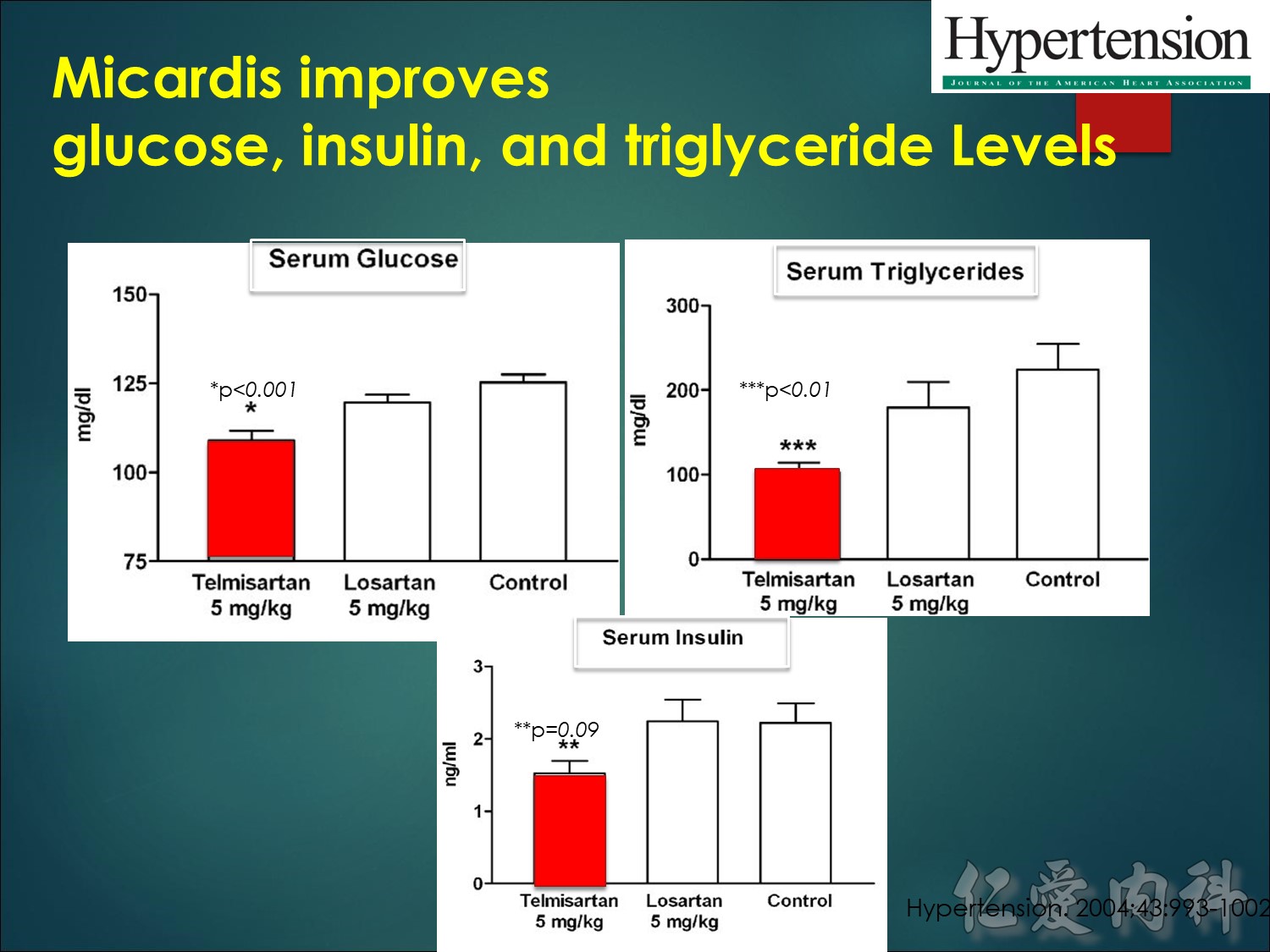
經過5週的餵食後,使用Telmisartan的老鼠,血清葡萄糖濃度明顯比使用Losartan的老鼠低,同時Telmisartan老鼠也顯示較低的血清胰島素濃度,雖然未達明顯差異的程度。葡萄糖與胰島素濃度的差異,證實Telmisartan具有優於Losartan的胰島素增敏性。另外,Telmisartan也能夠明顯降低三酸甘油脂的濃度,這樣的影響在Losartan老鼠身上也看不到。
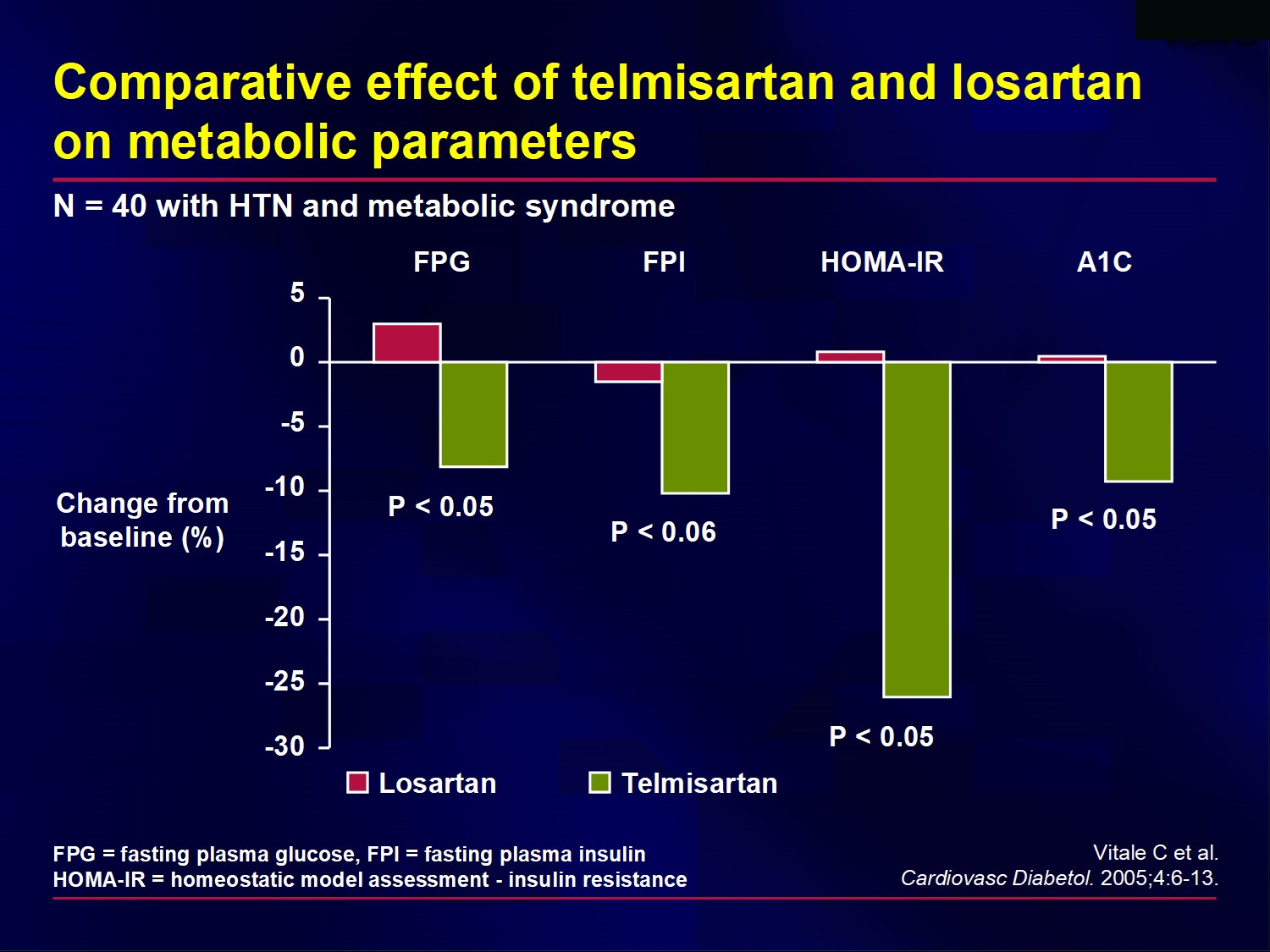
This study found that compared with once-daily losartan 50 mg, once-daily telmisartan
80 mg improved metabolic parameters in patients with metabolic syndrome, including glucose tolerance and insulin sensitivity.
Telmisartan reduced fasting plasma glucose by 8%, fasting plasma insulin by 10%, homeostasis model assessment (HOMA)-insulin resistance by 26%, and hemoglobin A1C by 9%. Losartan did not have a significant effect on these parameters.
The insulin-sensitizing activity displayed by telmisartan (but not by losartan) may be explained by its partial PPAR-gamma activity.
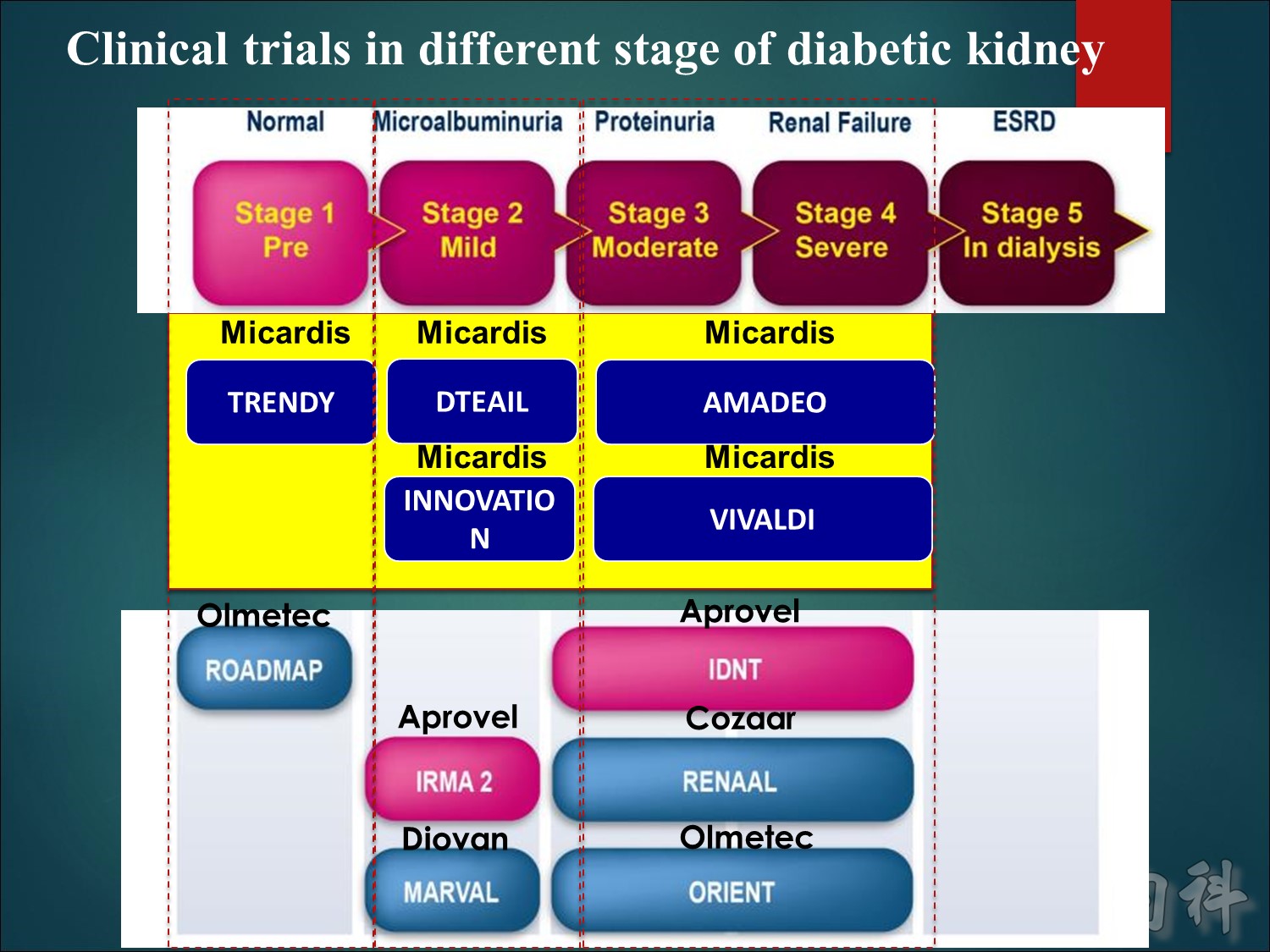
ROADMAP: 4447 patients with T2DM were assigned to receive olmesartan 40 mg/d or placebo for a median of 3.2 years. The primary outcome was the time to the first onset of MAU. IRMA 2: 590 hypertensive patients with T2DM and MAU were enrolled in this double-blind, placebo-controlled study of irbesartan, at a dose of either 150 mg/d or 300 mg/d, and were followed for 2 years. The primary outcome was the time to the onset of diabetic nephropathy. MARVAL: 332 patients with T2DM and MAU, with or without hypertension, were randomly assigned to 80 mg/d valsartan or 5 mg/d amlodipine for 24 weeks. The primary end point was the percent change in UAER from baseline to 24 weeks. IDNT: 1715 hypertensive patients with nephropathy due to T2DM were randomly assigned to irbesartan 300 mg/d, amlodipine 10 mg/d, or placebo. The primary end point was the composite of a doubling of the baseline serum creatinine concentration, the onset of ESRD, or death. RENAAL: 1513 patients were enrolled in this study comparing losartan (50 to 100 mg/d) with placebo for a mean of 3.4 years. The primary outcome was the composite of a doubling of the baseline serum creatinine concentration, ESRD, or death. ORIENT: The objective of study is to examine the effects of olmesartan on primary composite outcome of doubling of serum creatinine, ESRD and death in T2DM patients with overt nephropathy.
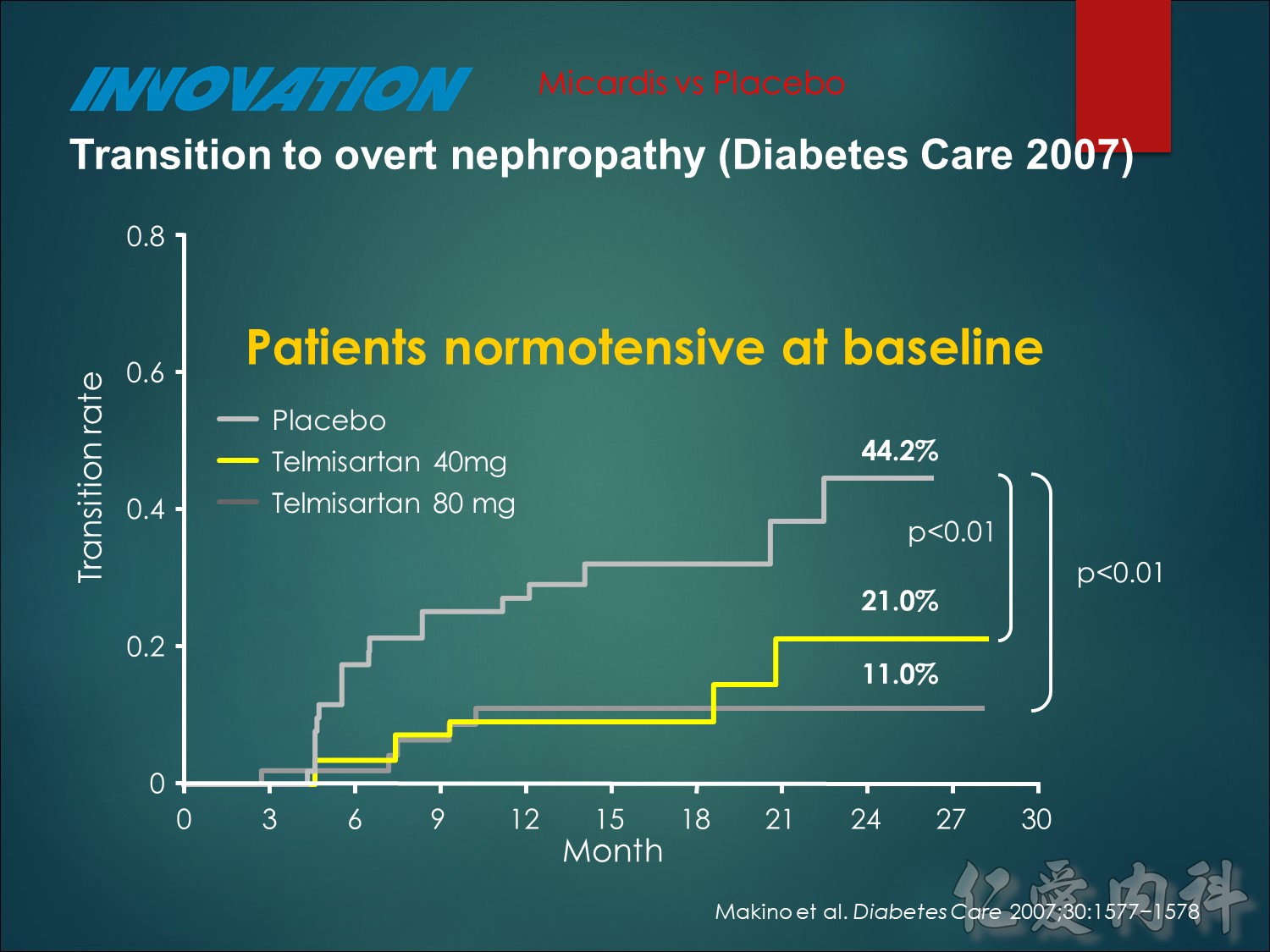
A total of 163 normotensive patients were included in the study.
Transition rates in normotensive patients were:
telmisartan 80 mg (n = 51) 11.0%
telmisartan 40 mg (n = 58) 21.0%
and placebo (n = 54) 44.2%
Makino H, et al. Prevention of transition from incipient to overt nephropathy with telmisartan in patients with type 2 diabetes. Diabetes Care 2007;30:1577−1578.
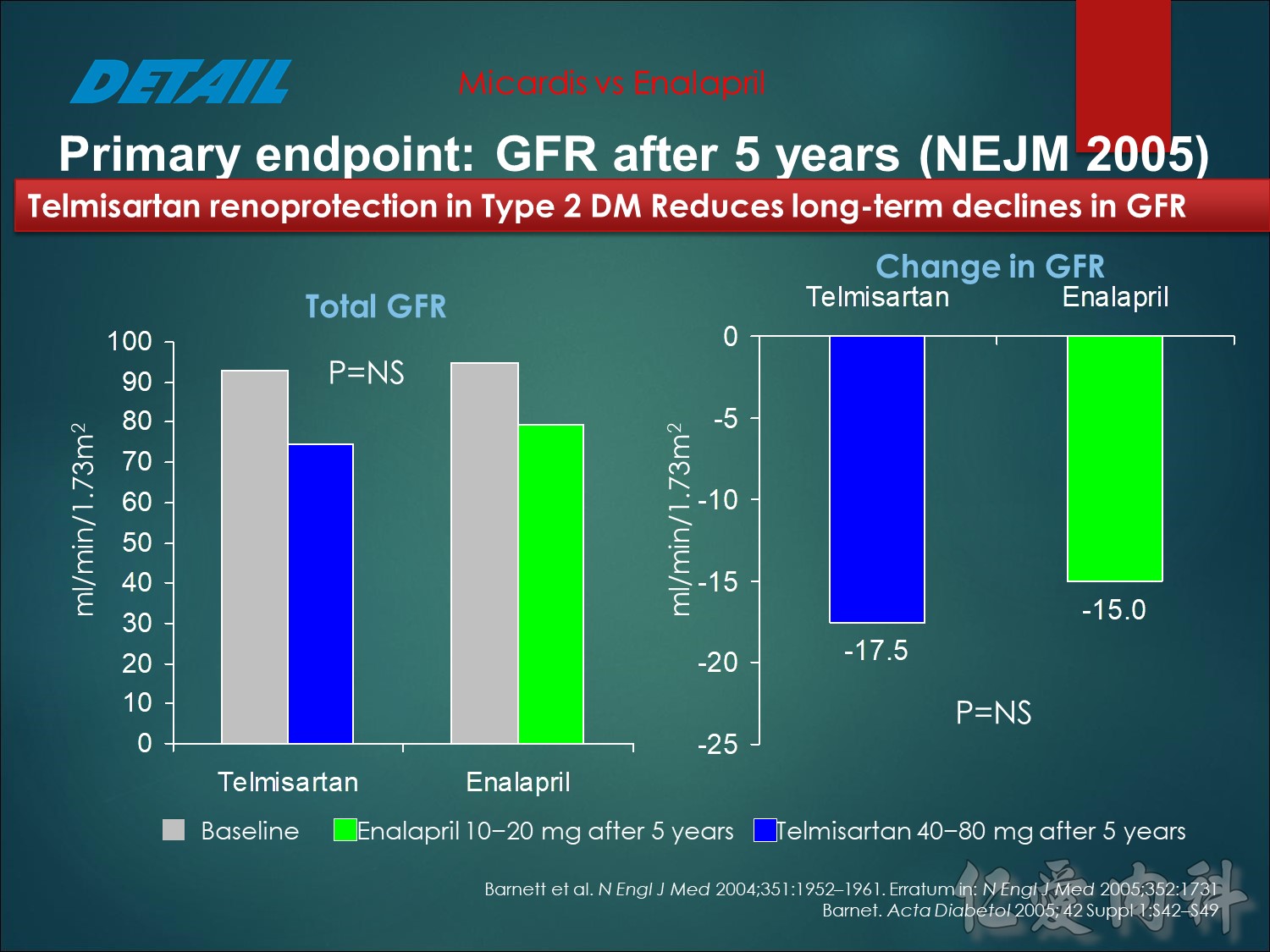
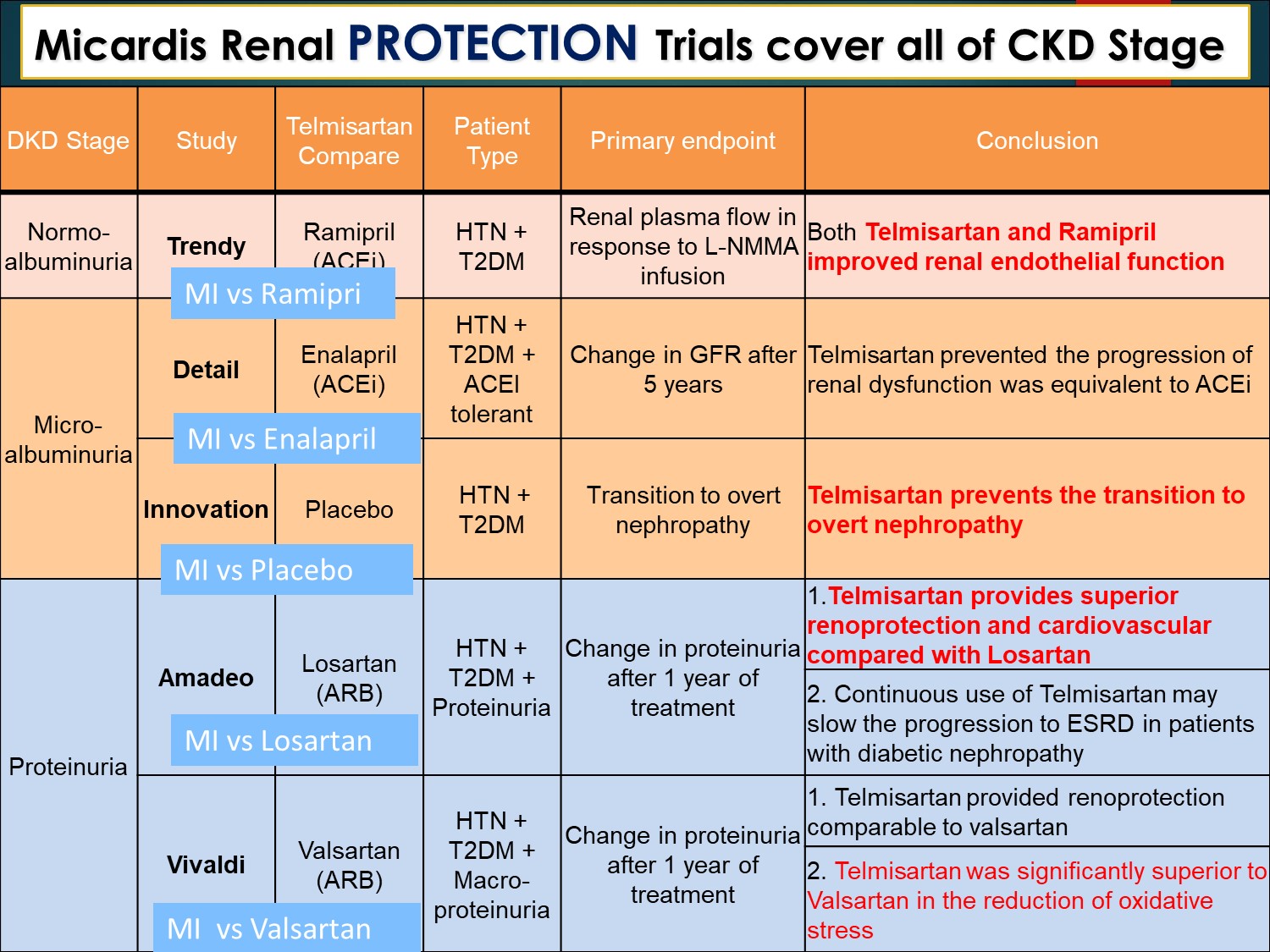
There were no significant differences in GFR at 5 years, or in the change in GFR over 5 years.1
At endpoint, the difference (telmisartan minus enalapril) in GFR was –2.6 ml/min/1.73 m2, with 95% confidence intervals (CIs) –7.1 to +2.0.
Telmisartan was comparable to enalapril (i.e., met the statistical test for non-inferiority), since the 95% CI of the difference was
≤10 mL/min/1.73m2.
1.Barnett A, et al. Angiotensin-receptor blockade versus converting-enzyme inhibition in type 2 diabetes and nephropathy. N Engl J Med 2004;351:1952–1961.
2.Barnett AH. Preventing renal complications in diabetic patients: the Diabetics Exposed to Telmisartan And enalaprIL (DETAIL) study. Acta Diabetol 2005;42 Suppl 1:S42–S49.
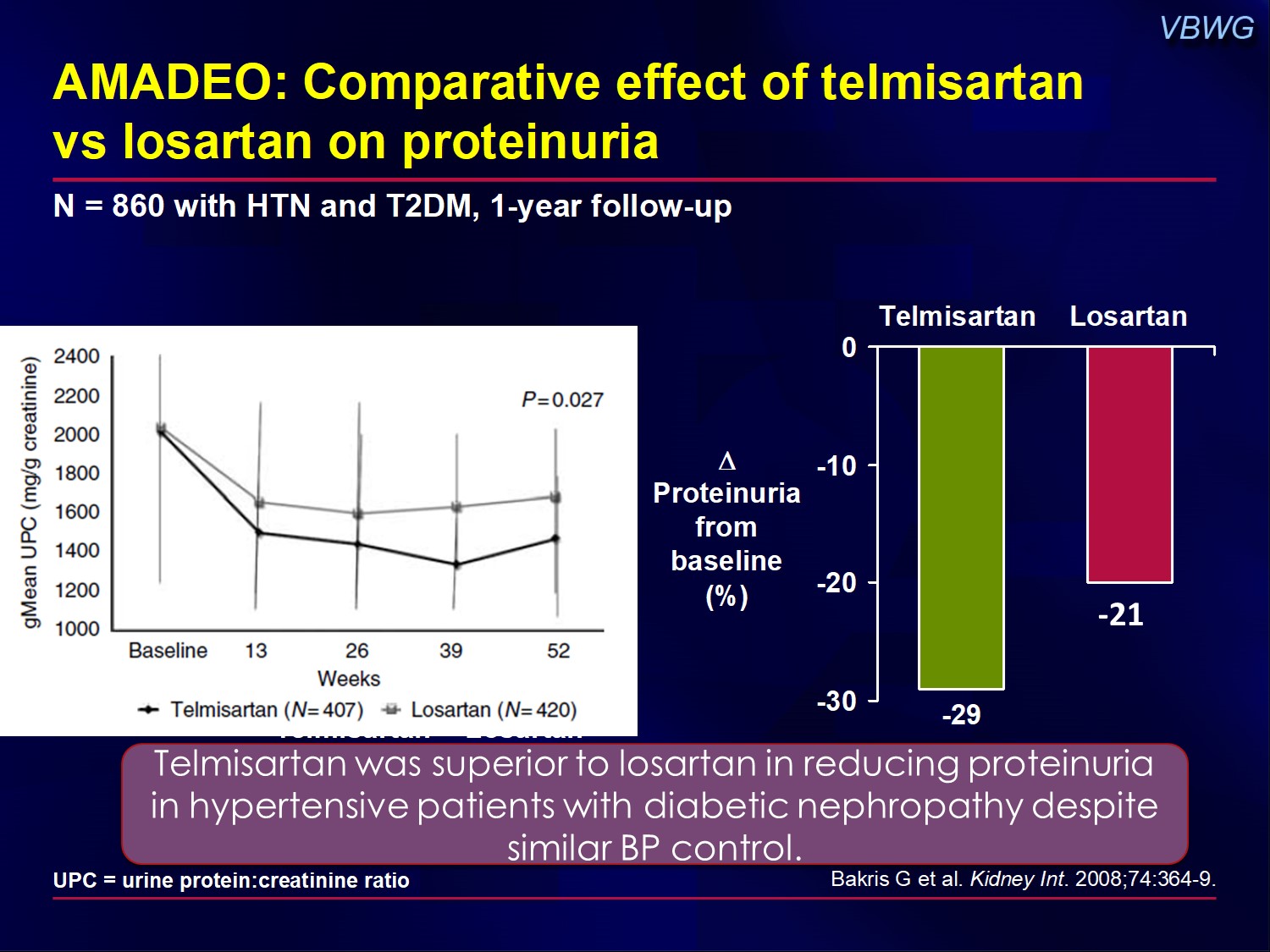
The AMADEO study compared the effects of telmisartan vs losartan on proteinuria in patients with T2DM, overt nephropathy, and hypertension.
One year of treatment with telmisartan provided greater reductions in proteinuria when compared with losartan, an ARB with an indication to slow diabetic nephropathy progression.
Telmisartan was superior to losartan in reducing proteinuria in hypertensive patients with diabetic nephropathy despite similar BP control.
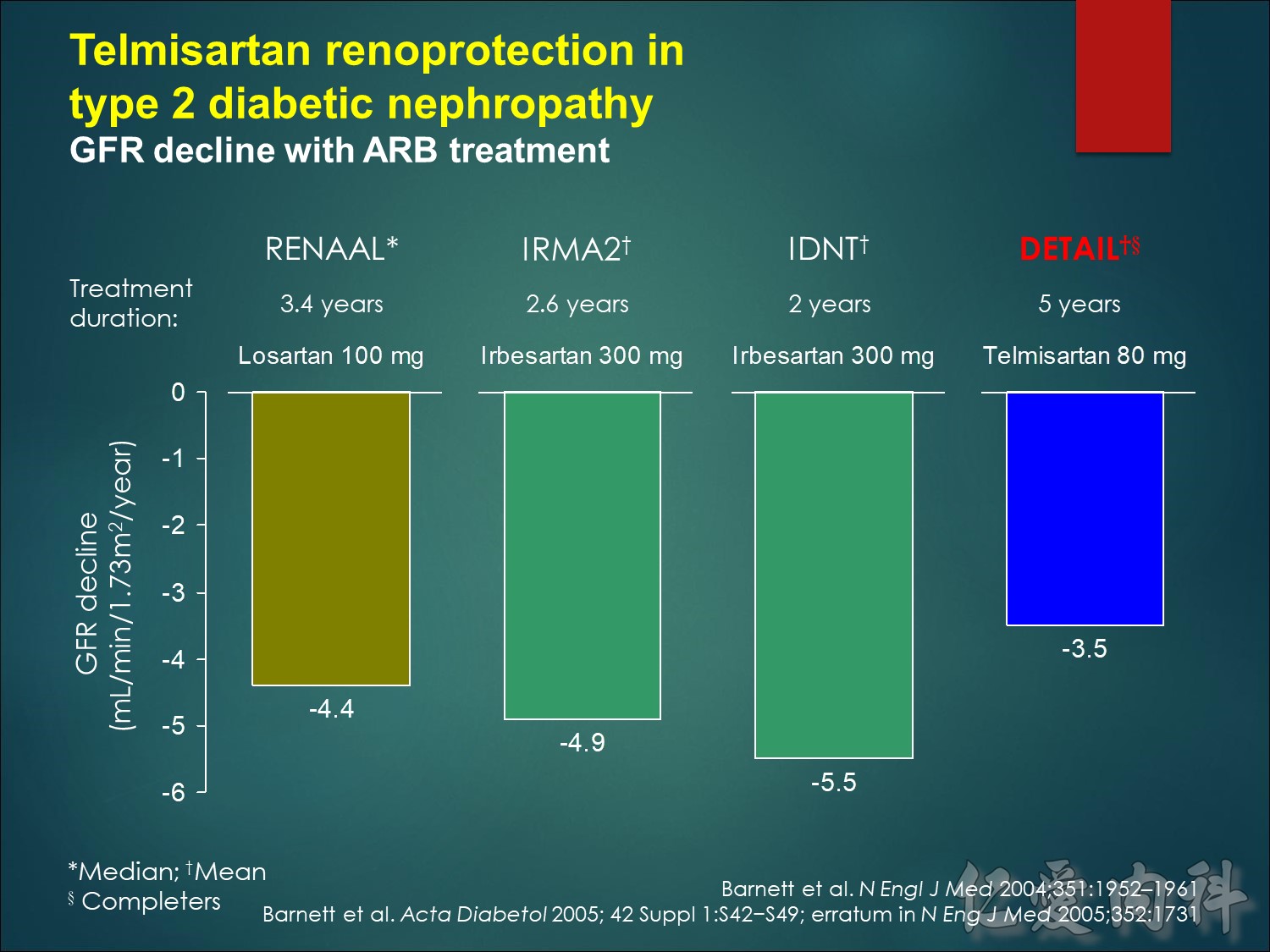
讓eGFR 下降少一點 腎保護效果
hours in IDNT). Patients in IRMA2 were similar to those in DETAIL
(baseline GFR = 109 ml/min/1.73m2, UAER 55 µg/min, SBP/DBP=153/90 mmHg).
The mean treatment duration was 3.4 years in RENAAL and 2.6 years in IDNT. IRMA2 was a 2-year study.
1.Barnett A, et al. Angiotensin-receptor blockade versus converting-enzyme inhibition in type 2 diabetes and nephropathy. N Engl J Med 2004;351:1952–1961.
2.Barnett AH. Preventing renal complications in diabetic patients: the Diabetics Exposed to Telmisartan And enalaprIL (DETAIL) study. Acta Diabetol 2005;42 Suppl 1:S42–S49; erratum in N Eng J Med 2005;352:1731.