作者/講者: 黃庭章 醫師
整理: Ian YC Chen, MD
校稿: Ian YC Chen, MD
上次校閱: 2018/04/07

Inflammatory Bowel Disease
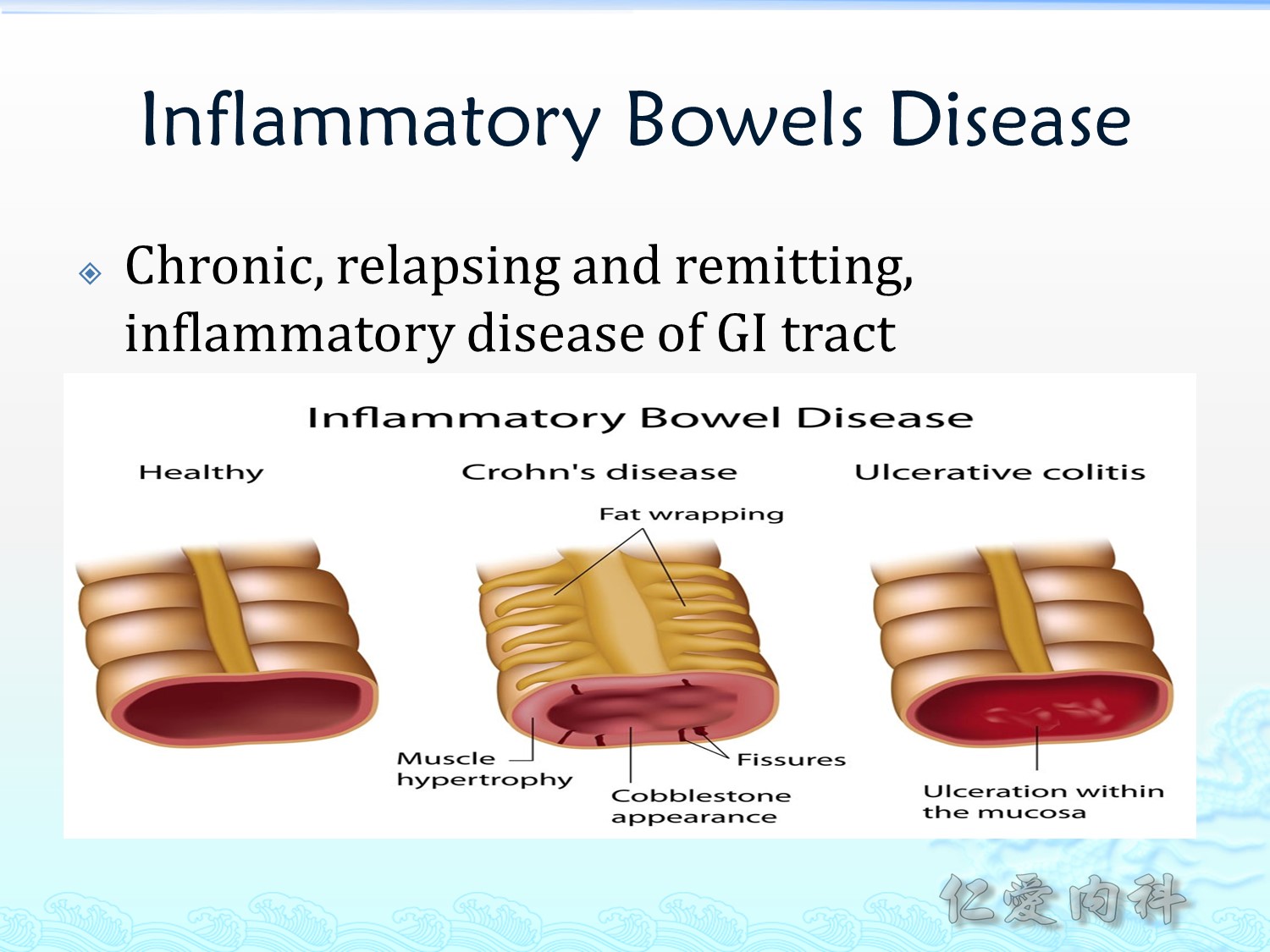
Inflammatory bowel disease 是一類慢性反復性的腸胃道發炎性疾病。其主要分為兩個疾病:
- Crohn’s disease:主要是 transmural invasion, 所以常常會造成 fissures 或是 strictures, 或是內視鏡檢查下可見到 cobblestone 的表現。
- Ulcerative colitis:主要侵犯大腸, 特別是黏膜層, mucosal layer。

Inflammatory bowel disease 在歐美國家盛行率較高,亞洲國家較低。看起來似乎也與國家的開發程度有關。
Inflammaotry bowel disease 的 onset 年齡為 20-40 歲,約有 15% 的病人在 60 歲之後發病,稱為 older-onset IBD (click to show the reference)。
{kind=link}
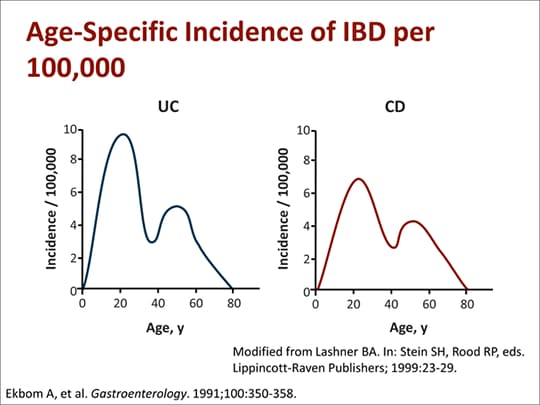
Ulcerative colitis 的 peak onset 的年齡約是 30-40 歲,Crohn’s disease 約比 ulcerative colitis 早10歲。兩者的第二個發生的年齡範圍大約是 60 歲之後。
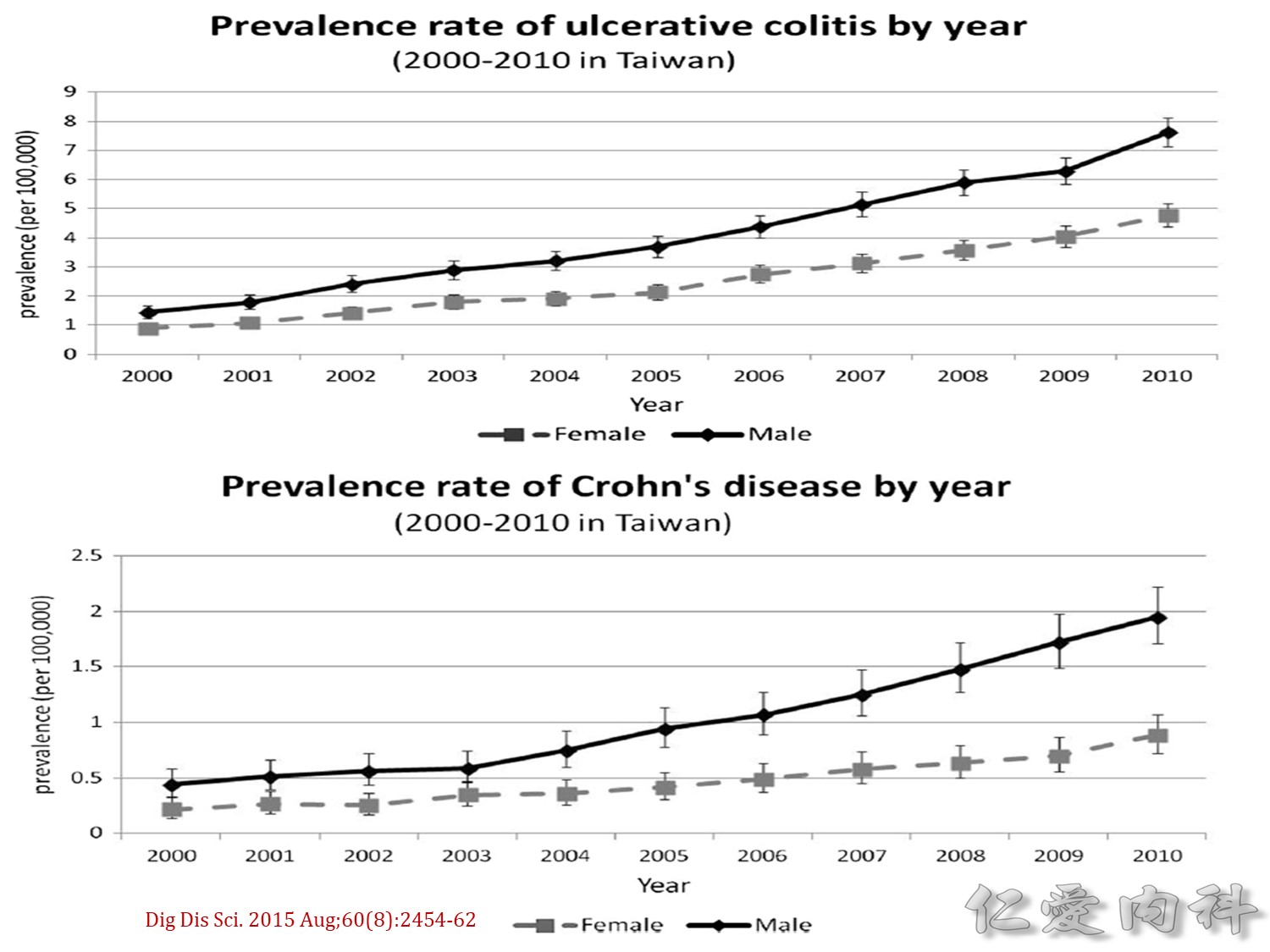
台灣的 IBD 盛行率是逐年上升 (2000-2010),可能與環境變遷的相關因素 (例如:飲食或藥物的使用) 有關。
UC 的病人比 CD 的病人多。
男性比女性多。
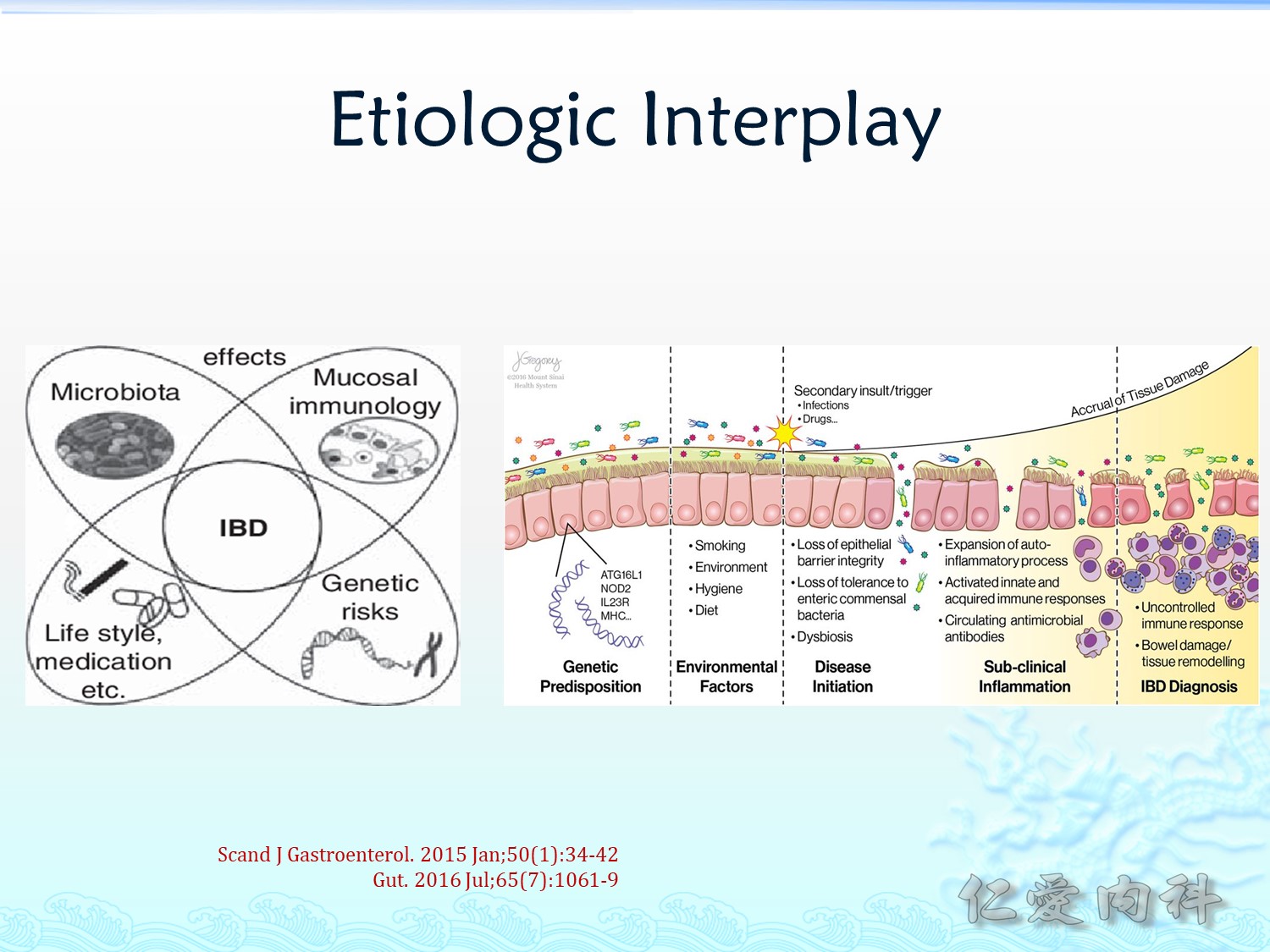
IBD 的 etiology 相當複雜,包含:
- genetic risks (ATG16L1, NOD2, IL23R, MHC…)
- lifestyle/medication (抽菸、早期接觸抗生素等)
- mucosal immunology
- microbiota
種種因素造成 mucosal barrier 的受損、感染、乃至全面失控的免疫反應進一步加重腸道組織的傷害。

左圖為正常狀況下 (eubiosis),腸道內的正常菌種能提供保護腸道免於受致病菌的侵害並能教育腸道免疫細胞。
但若是腸道菌的分佈被環境因素 (eg, antibiotics) 改變時 (dysbiosis),TH1、TH2、TH9、TH17、Neutrophils 等免疫細胞便會參與並改變原有的免疫調節與平衡。
Ulcerative Colitis
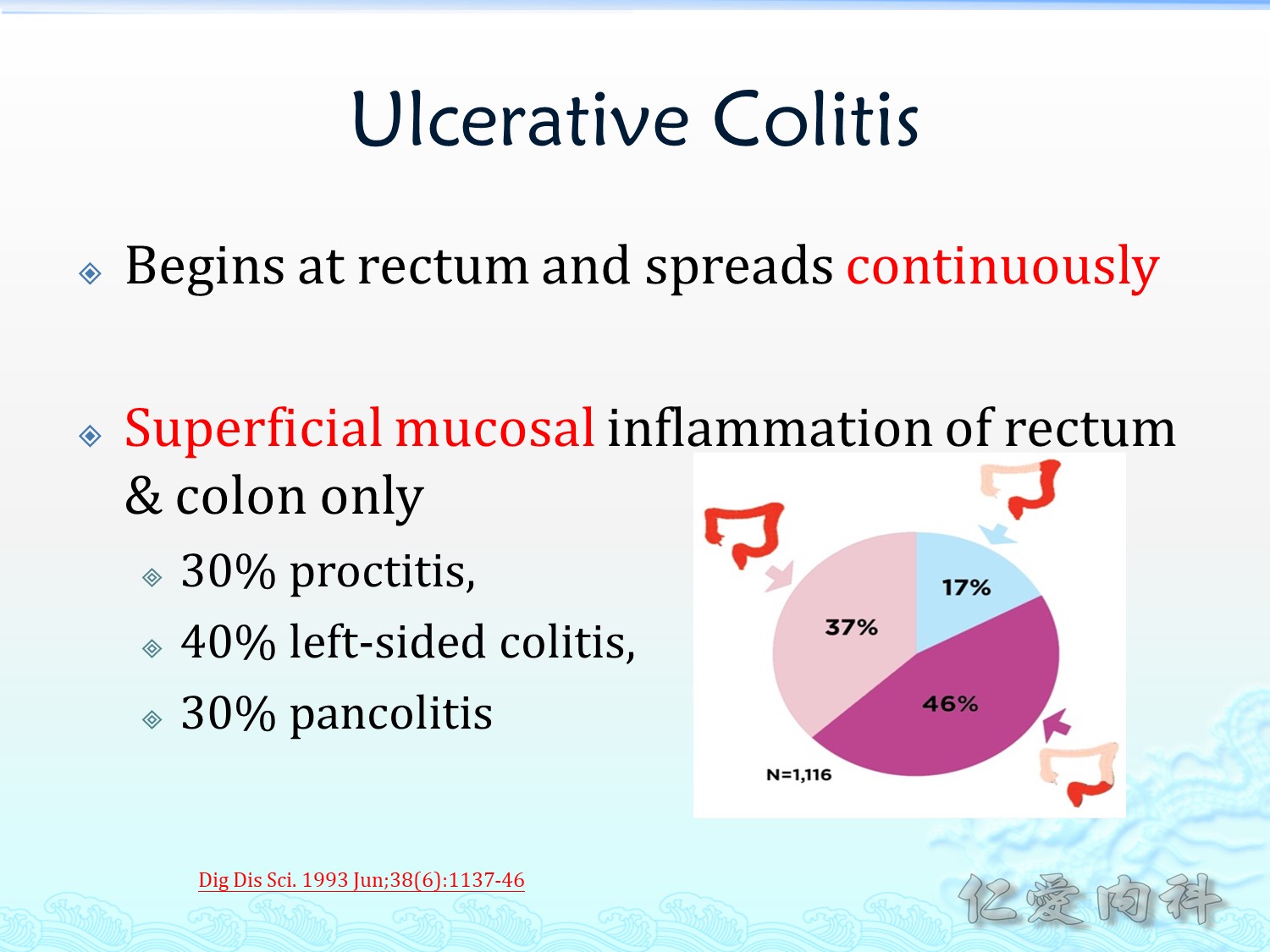
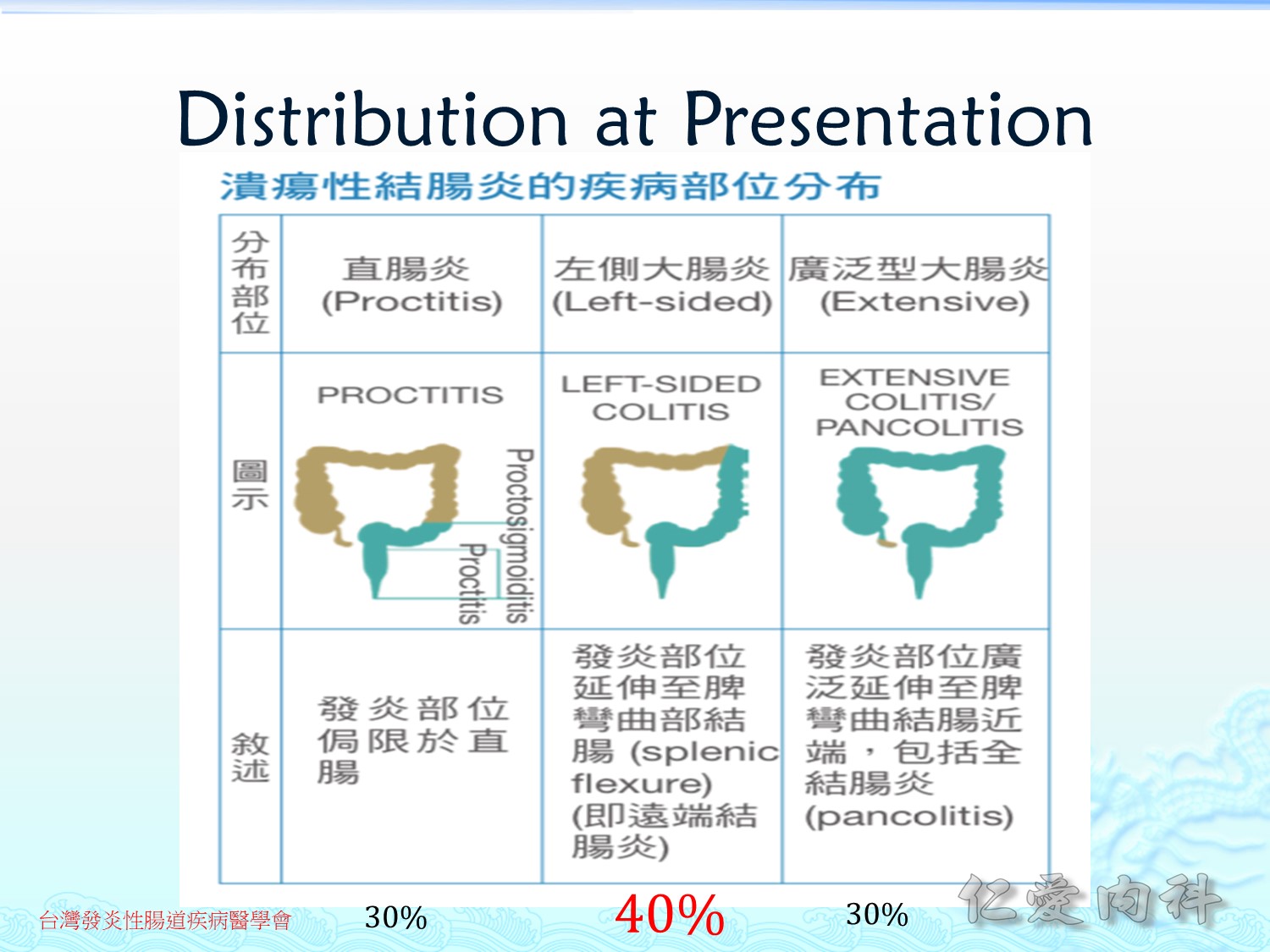
Ulcerative colitis 侵犯為連續性的且表淺的 (continunous and superficial),早期統計約 30% 為 proctitis / 40% 為 left-sided colitis / 30% 為 pancolitis,但是 (右圖) 最近的統計可以看出一些變化,left-sided colitis 明顯減少,而 proctitis明顯增加。
最常見的臨床表現為 chronic diarrhea,也可能有發燒、體重減輕、體力變差。
1/3的病人會有腸道外症狀 (extra-intestinal menifestations)。
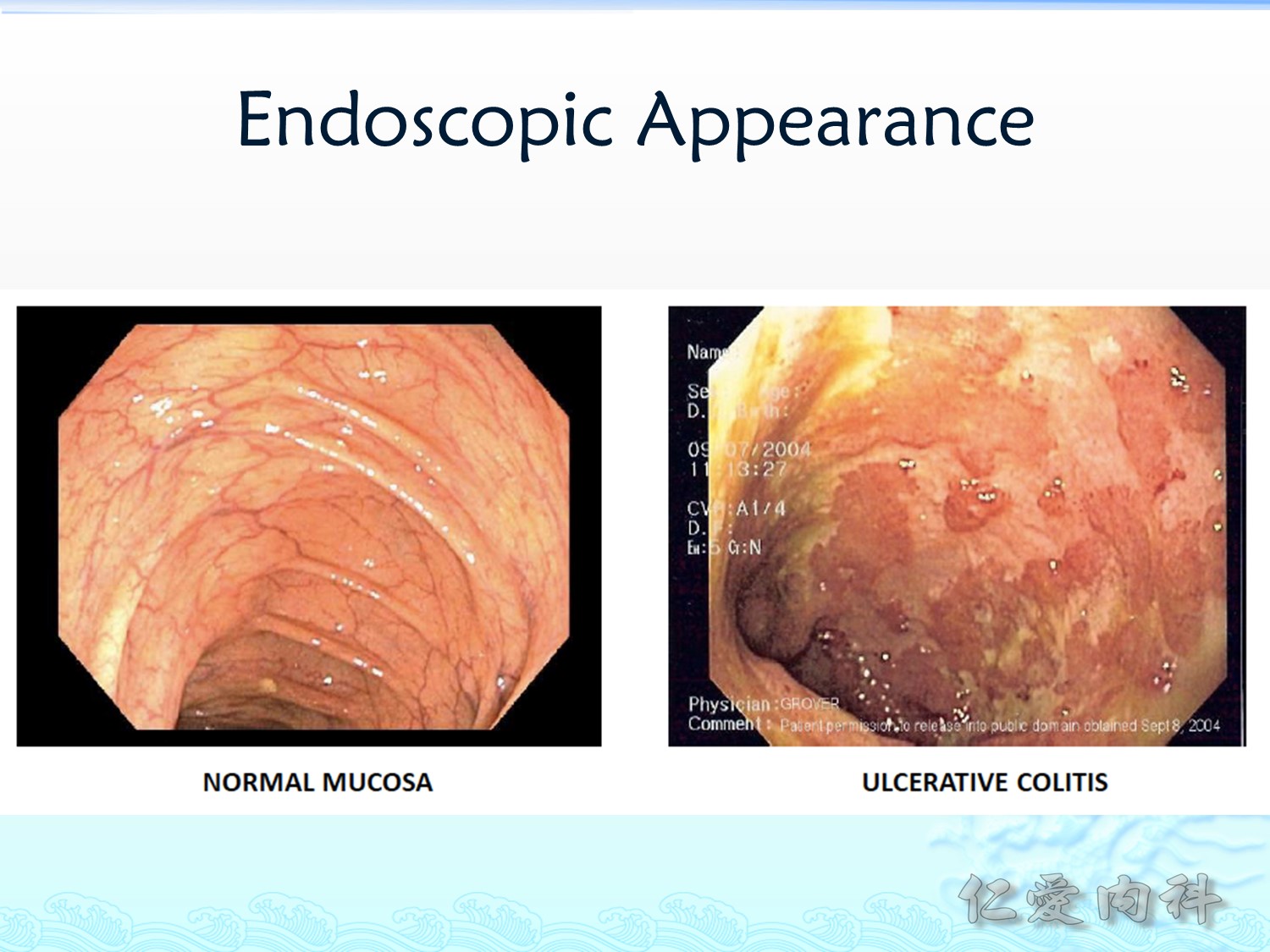
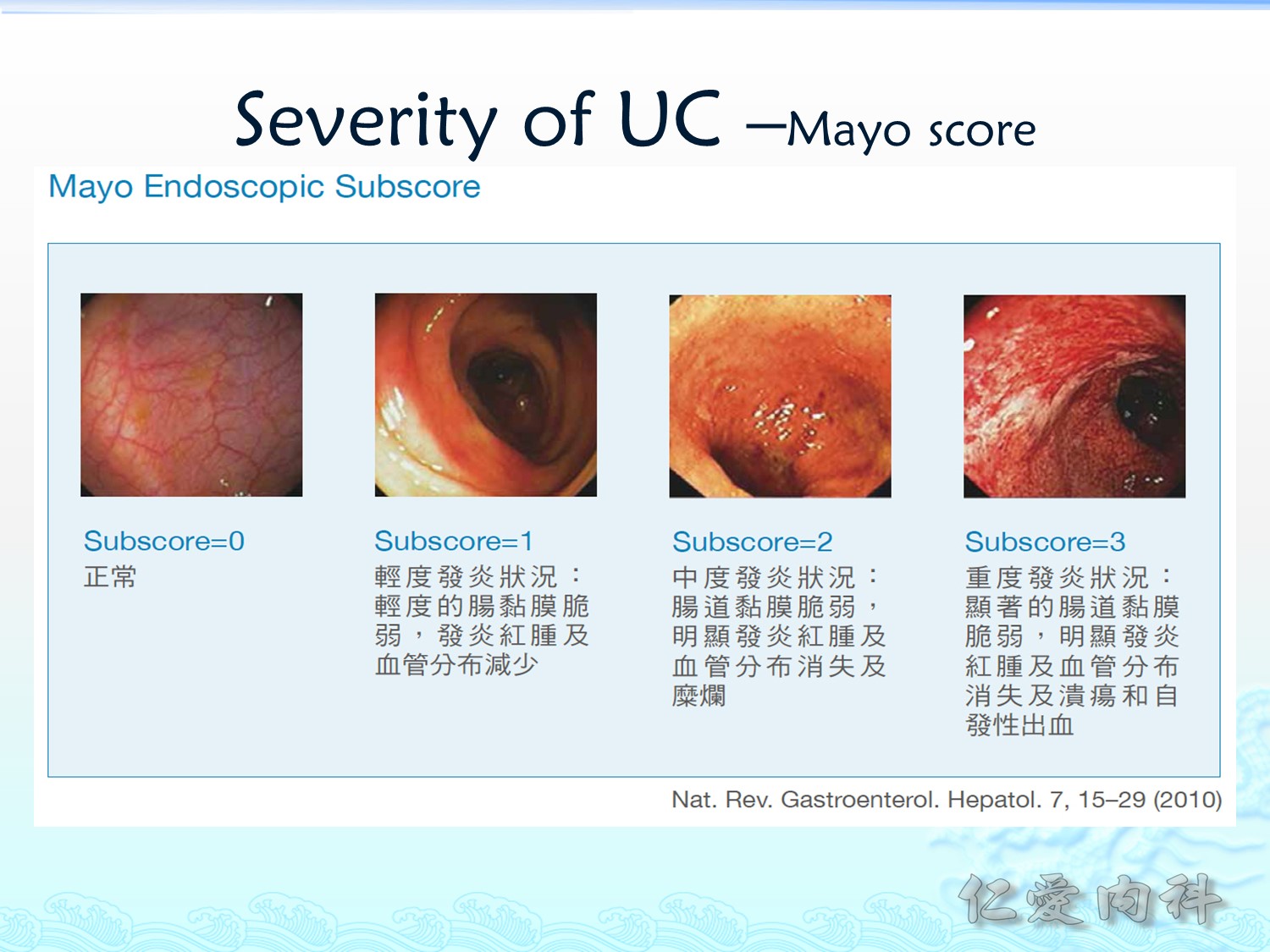
Ulcerative colitis 嚴重時 (右圖) 在內視鏡下可見到正常血管紋路消失、黏膜腫脹、以及 shallow ulcers。
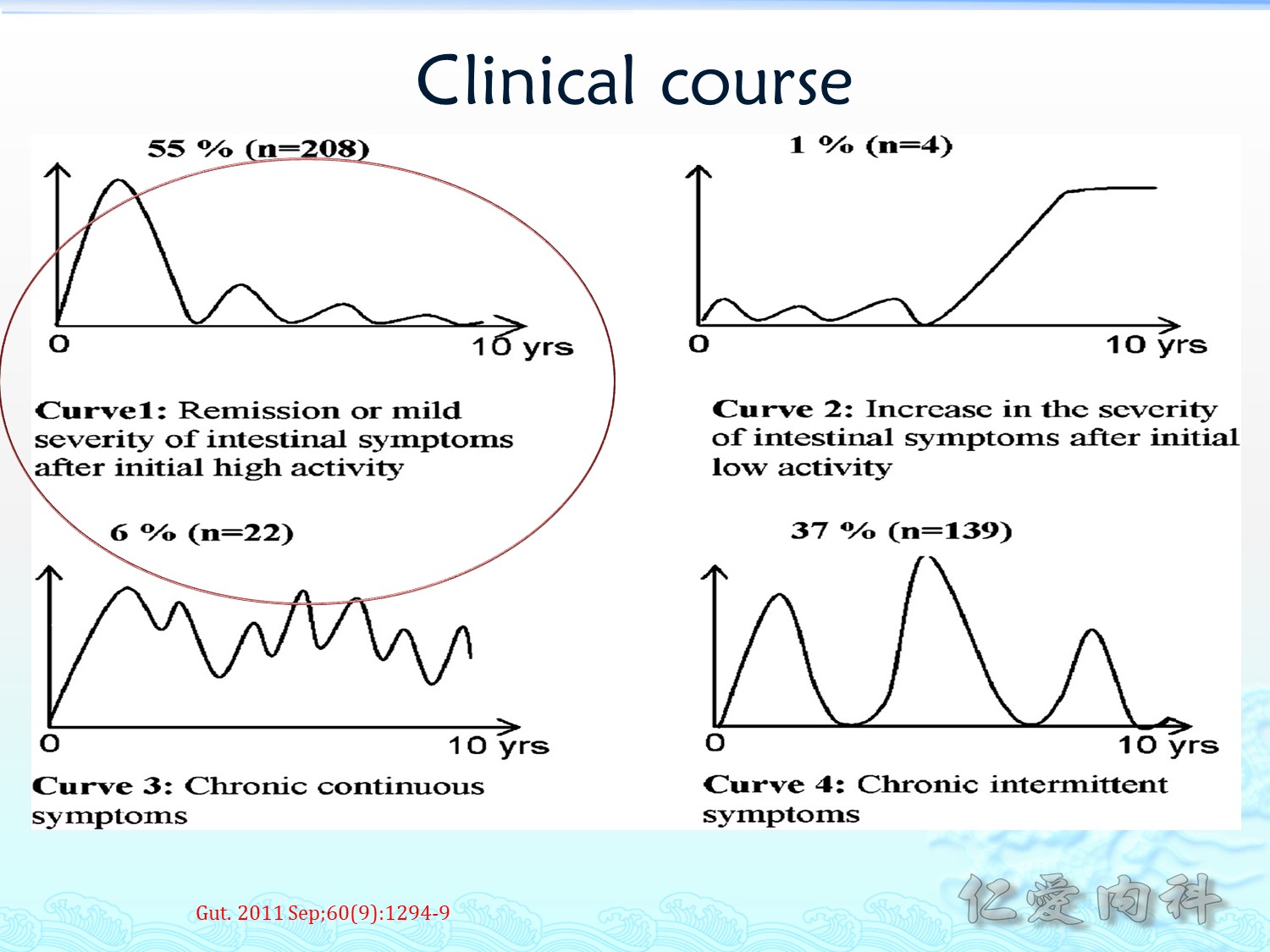
最常見的 clinical course (約60%) 為一次大的 flare-up 之後,有一些斷斷續續的小的輕微的腸道症狀;
其次常見的 clinical course (約40%) 為反復的 (intermittent) 慢性的 (chronic) 疾病症狀 (flare-ups 與remissions 交替出現)。
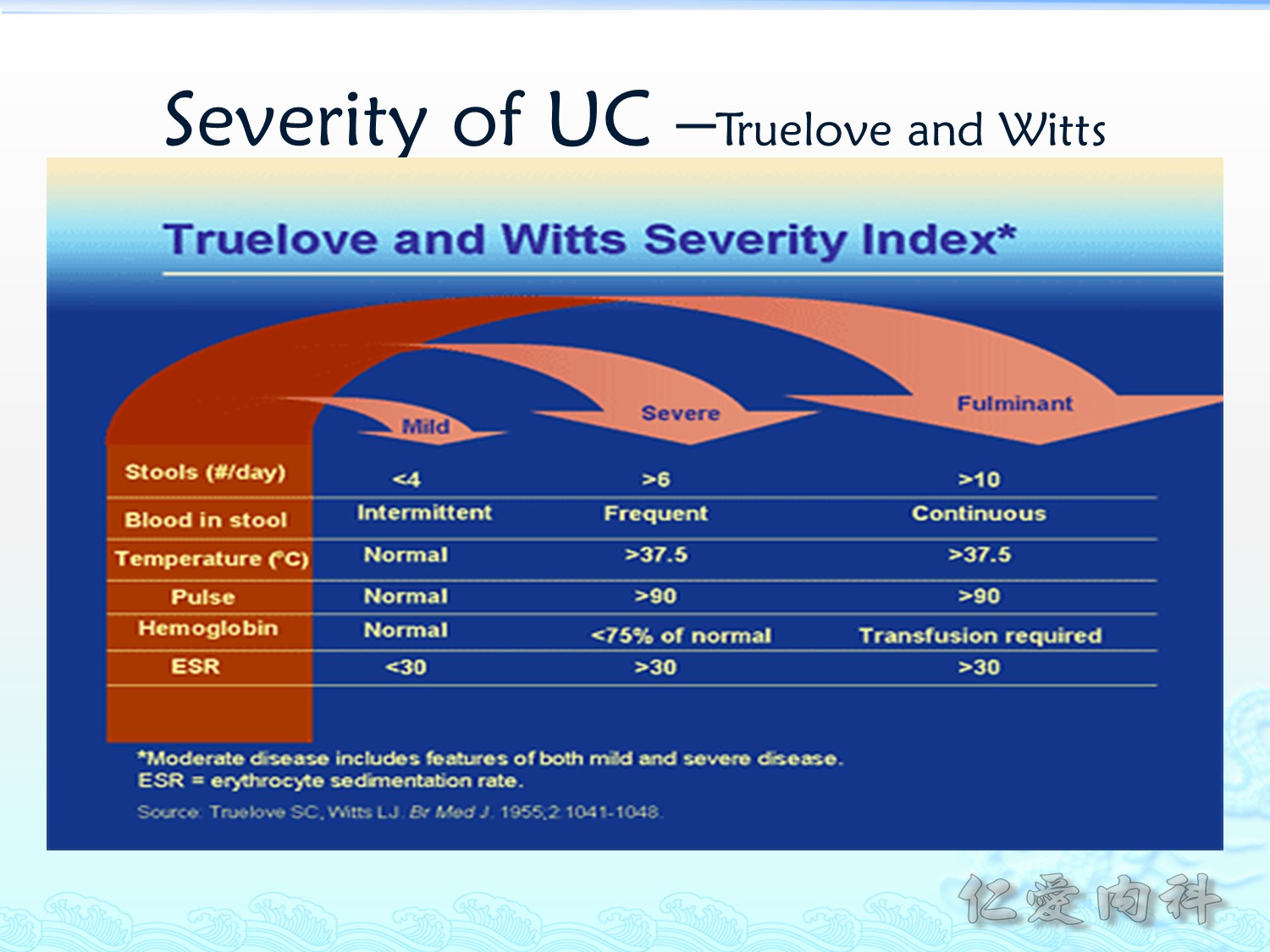
1995年提出的疾病嚴重程度評估工具—Truelove and Witts Severity Index
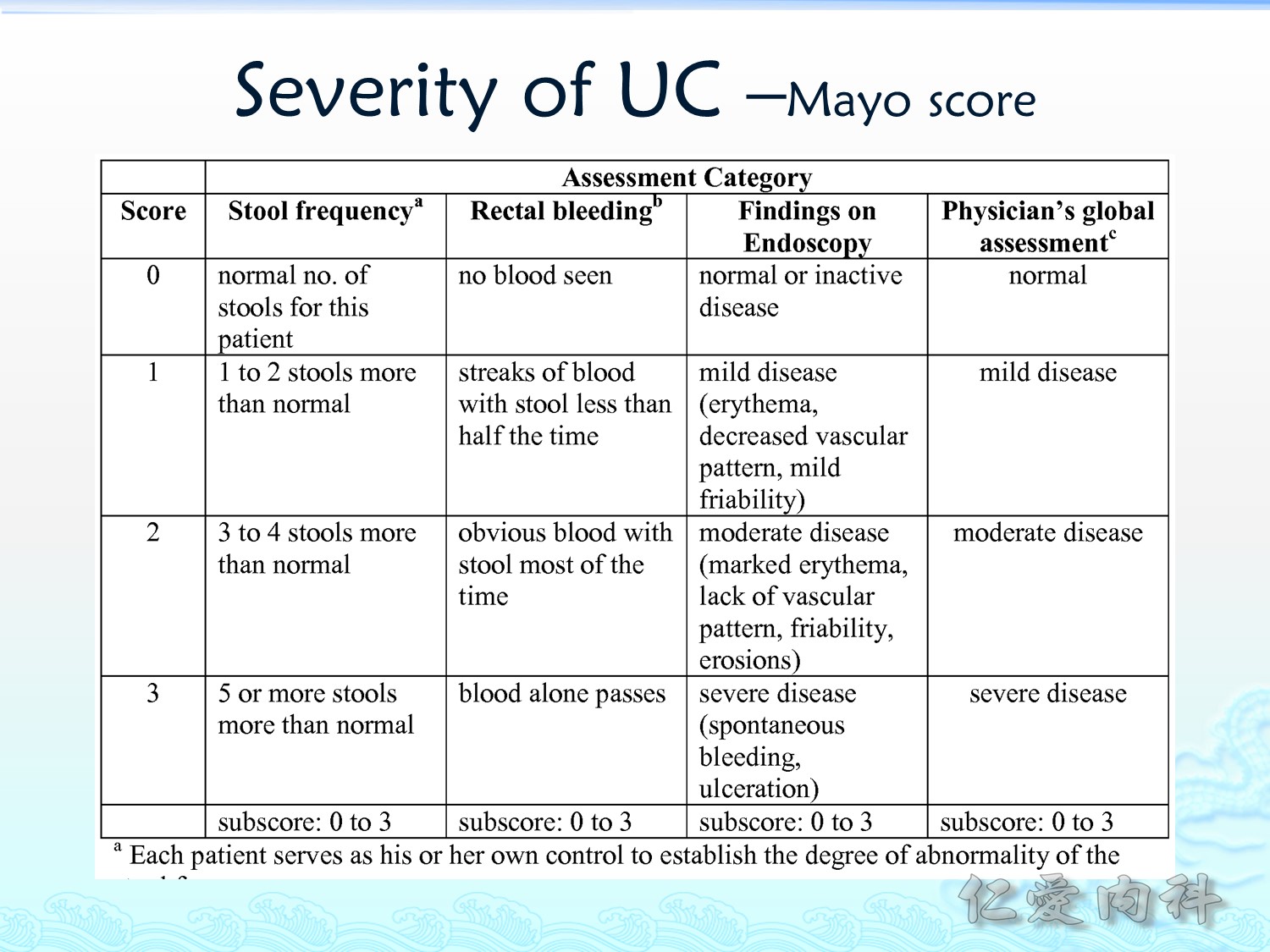
目前較常用的 UC 嚴重度評估工具為 Mayo score,其評估的指標有四項 (subscores):stool frequency, retal bleeding, endoscopic findings, physician’s global assessment
Crohn’s Disease
Crohn’s disease 的疾病特色為 transmural, skipped, noncaseating granulomatous (此點在亞洲區或 tuberculosis 盛行區域非常重要, 要與 intestinal tuberculosis 鑑別診斷)。
從嘴巴至直腸都可被侵犯。
Transmural invasion 容易造成一些 complications: 特別是 fistulas。
臨床表現與 UC 有些不同,主要是以腹痛而言,特別是右下腹;常有 diarrhea,但與 UC 不同的是不常有 bloody;也會有腸道外症狀。
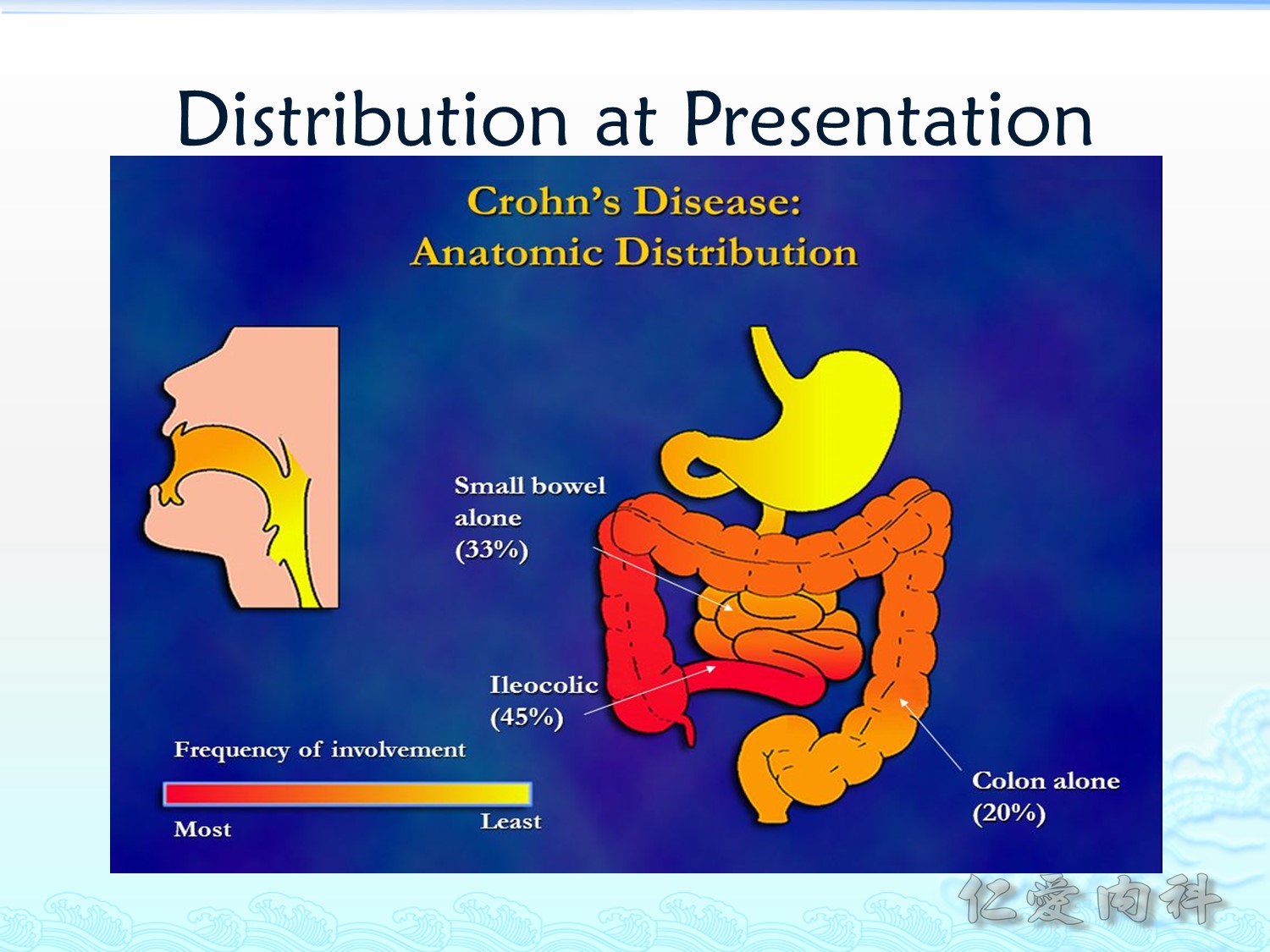
Crohn’s disease 有 45% 會侵犯 ileocolic (terminal illium 附近),因此會有右下腹痛;1/3 只侵犯小腸;20% 只侵犯大腸。

內視鏡下與 UC 不同的是 ulcer 為直線型的 (longitudinal),發炎嚴重時會產生 cobblestone appearance。

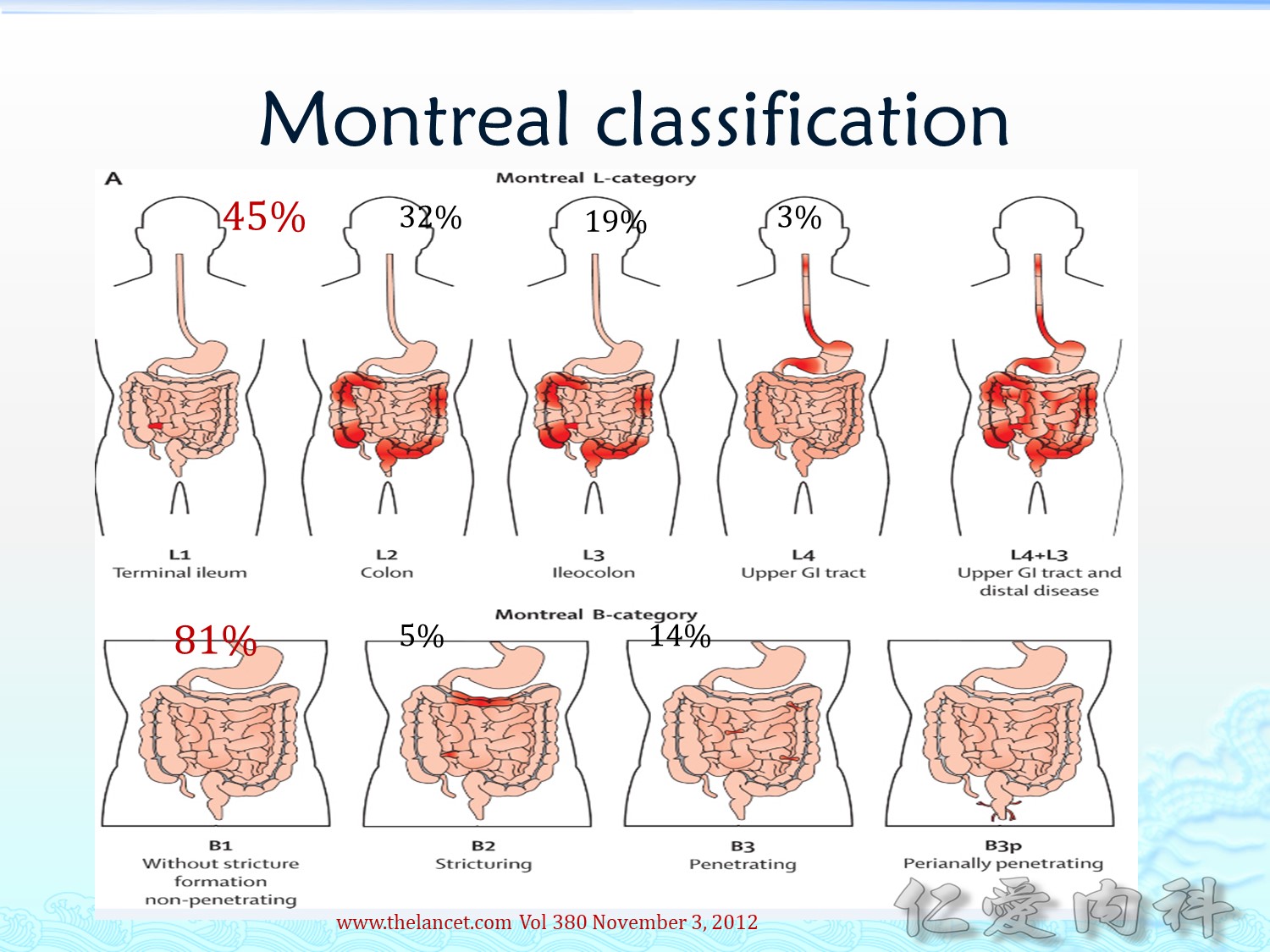
In 2000 the Vienna classification was introduced, which was the first attempt to classify different clinical phenotypes of CD. The Vienna classification was followed by the Montreal classification in 2008. The Montreal classification describes the extent and behaviour of CD in more detail and includes a classification system for UC.
CONCLUSION: We found a good to excellent inter-observer agreement for all Montreal items except for disease severity in UC (poor).
World J Gastroenterol. 2014 Nov 7; 20(41): 15374–15381.
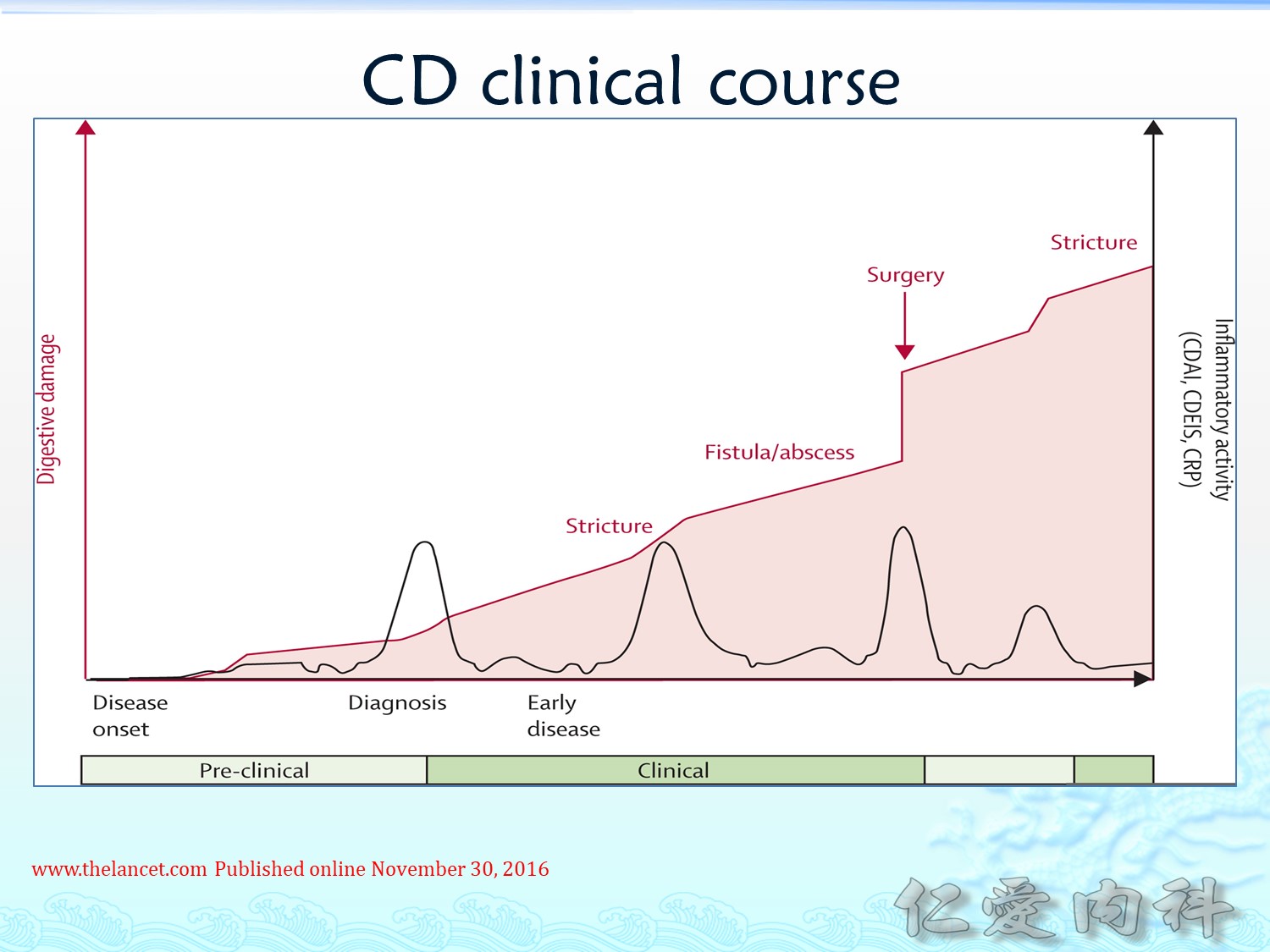
病人常有 flare-ups 與 remissions 乃至最後需要接受多次手術來緩解症狀 (手術切除不是 curative therapy)。
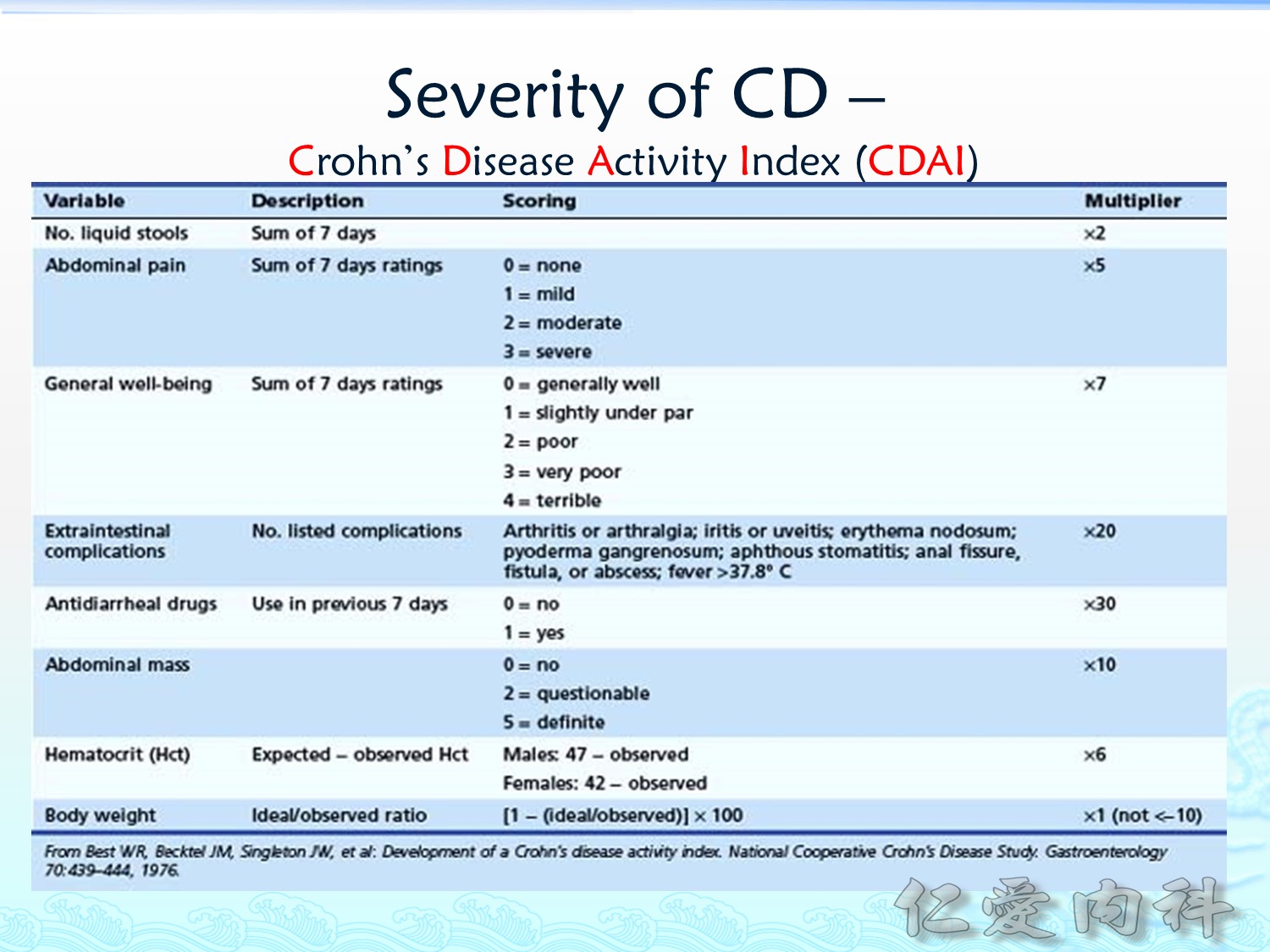
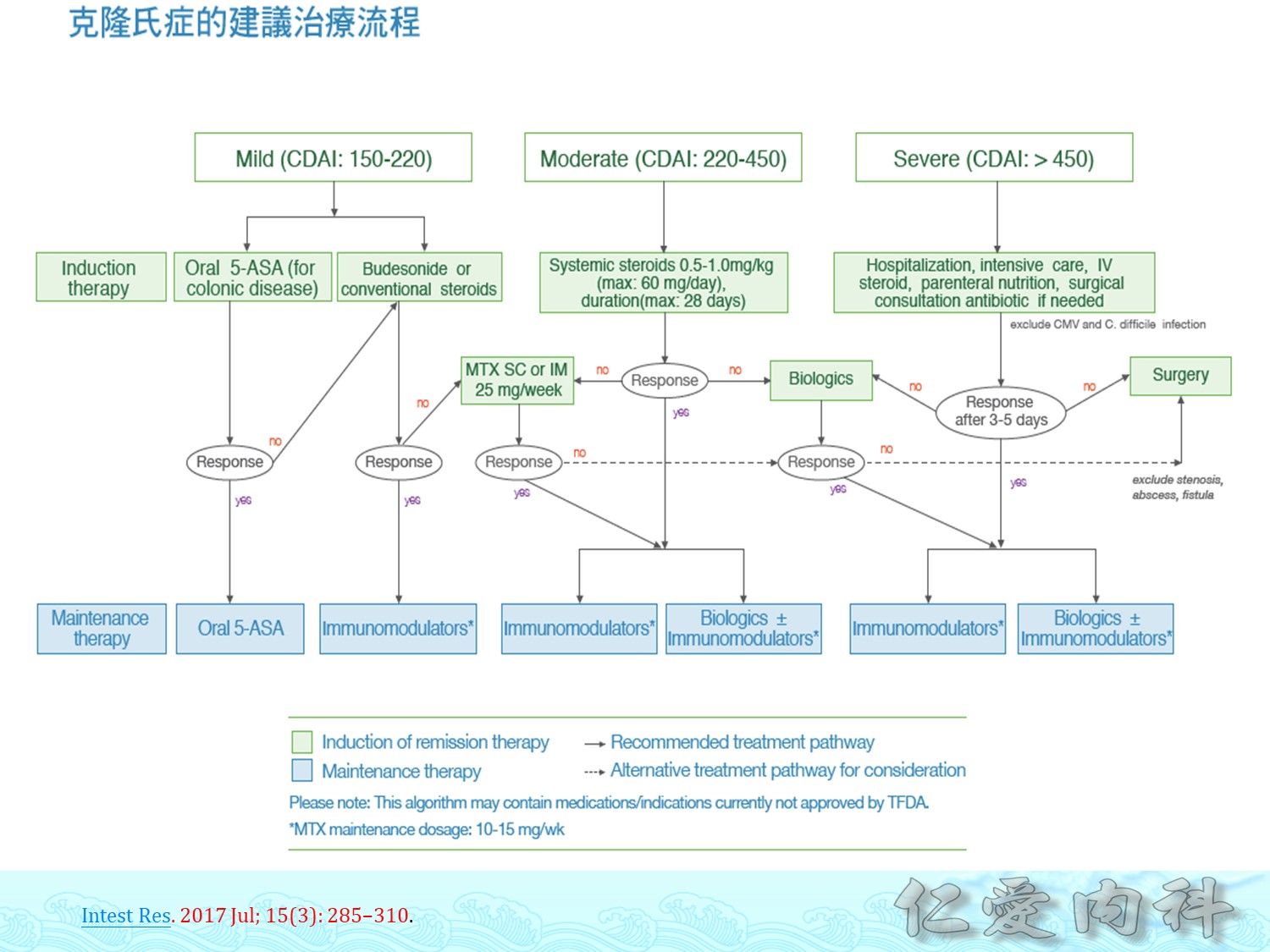
嚴重程度評估可用Crohn’s Disease Activity Index (CDAI)
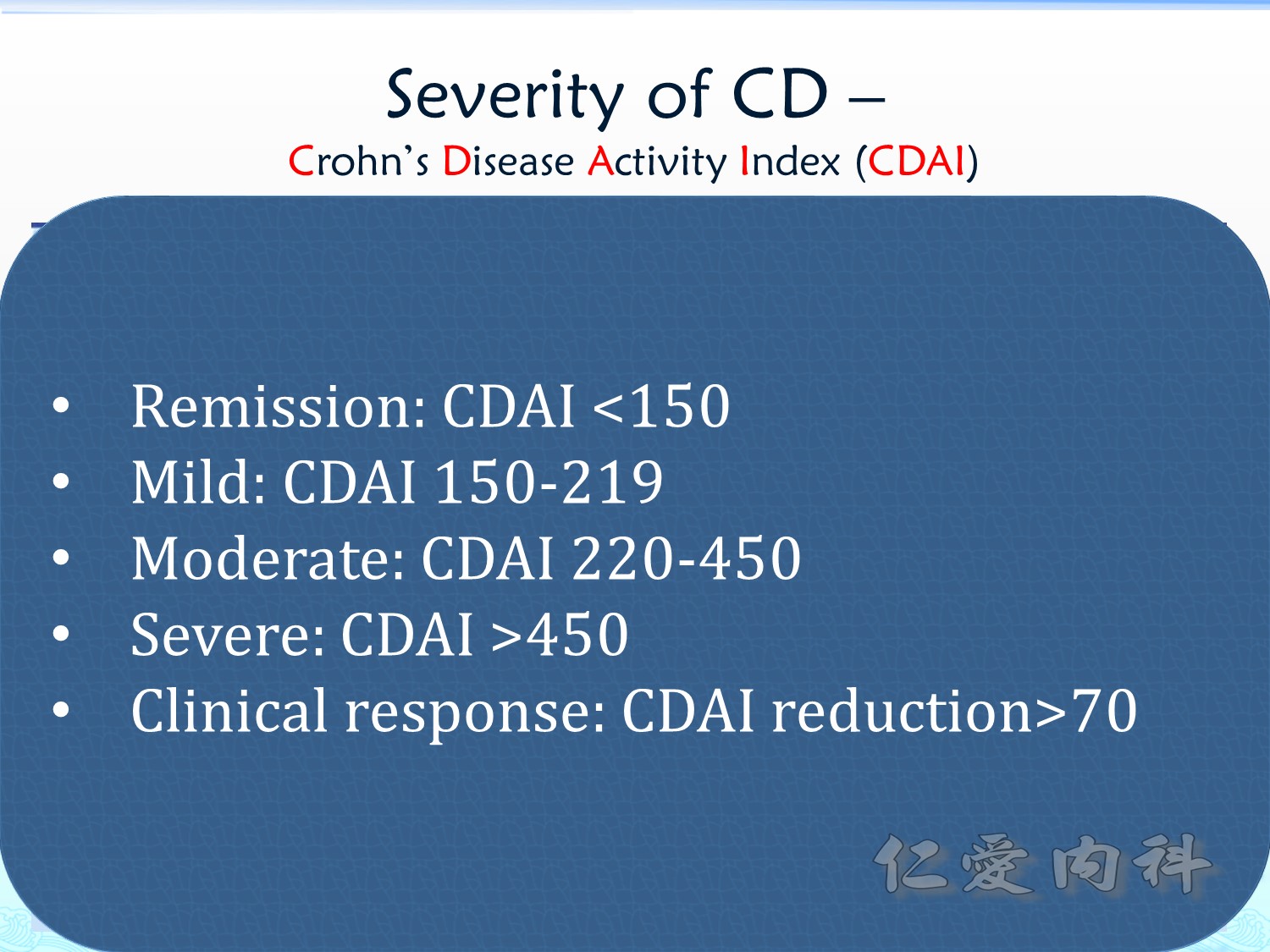 CDAI < 150 時表示為 remission。
CDAI < 150 時表示為 remission。
治療前後之 CDAI 減少超過 70 表示對於治療是有反應的。
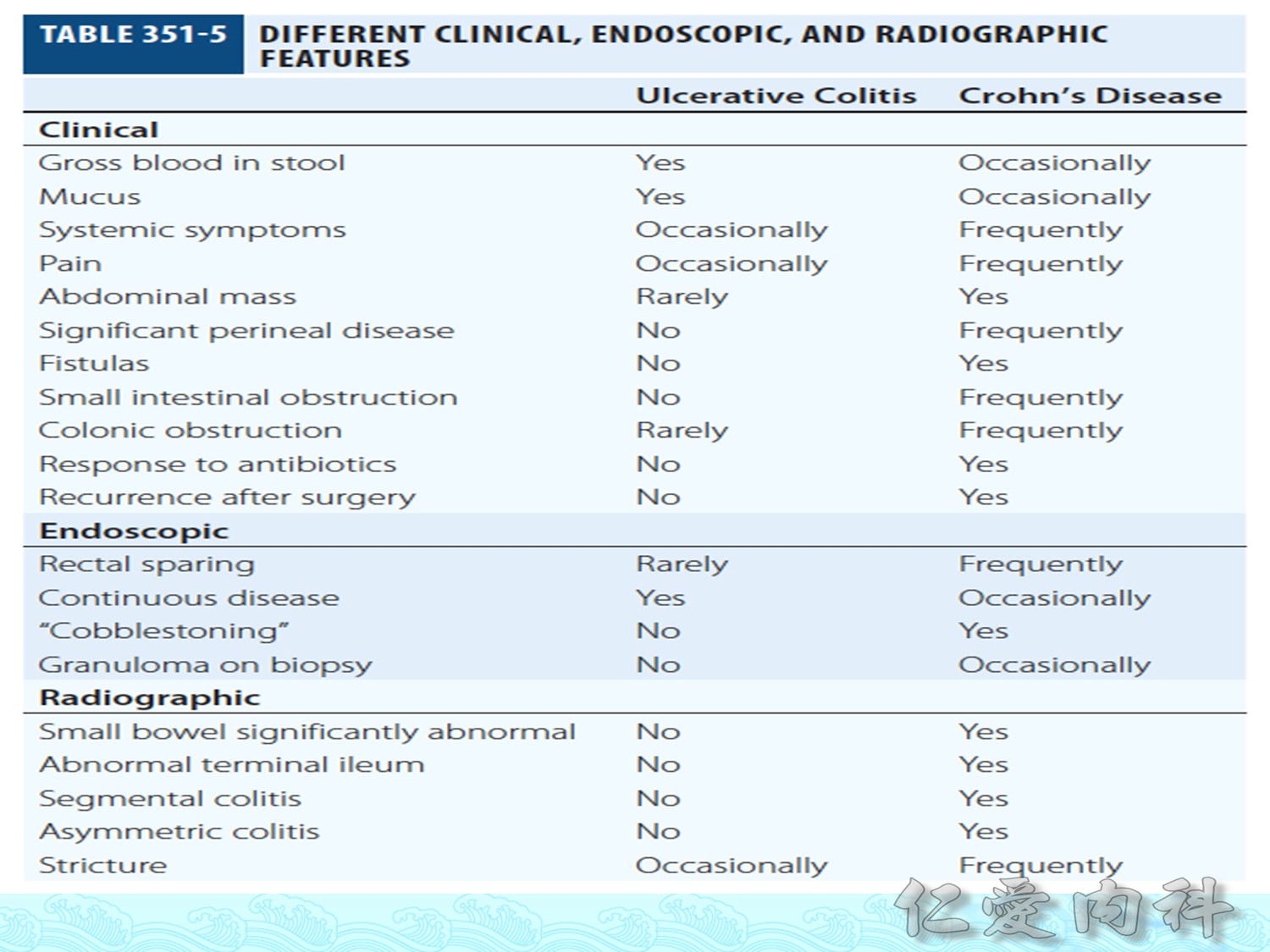
比較與整理 ulcerative colitis 與 Crohn’s disease
|
Ulcerative Colitis |
Crohn’s Disease |
|
Continuous/superficial |
“Skip lesions”/deep (transmural) |
|
Rectum to colon only |
Mouth to anus +/-rectum |
|
++Rectal bleeding |
+/-Rectal bleeding |
|
Rare strictures |
++Fistulas/strictures |
|
Surgery curative |
Surgery palliative (high rate of recurrence: >50%) |
|
Extra-intestinal manifestations |
Extra-intestinal manifestations |
|
Bloody diarrhea/urgency |
Abdominal pain/weight loss |
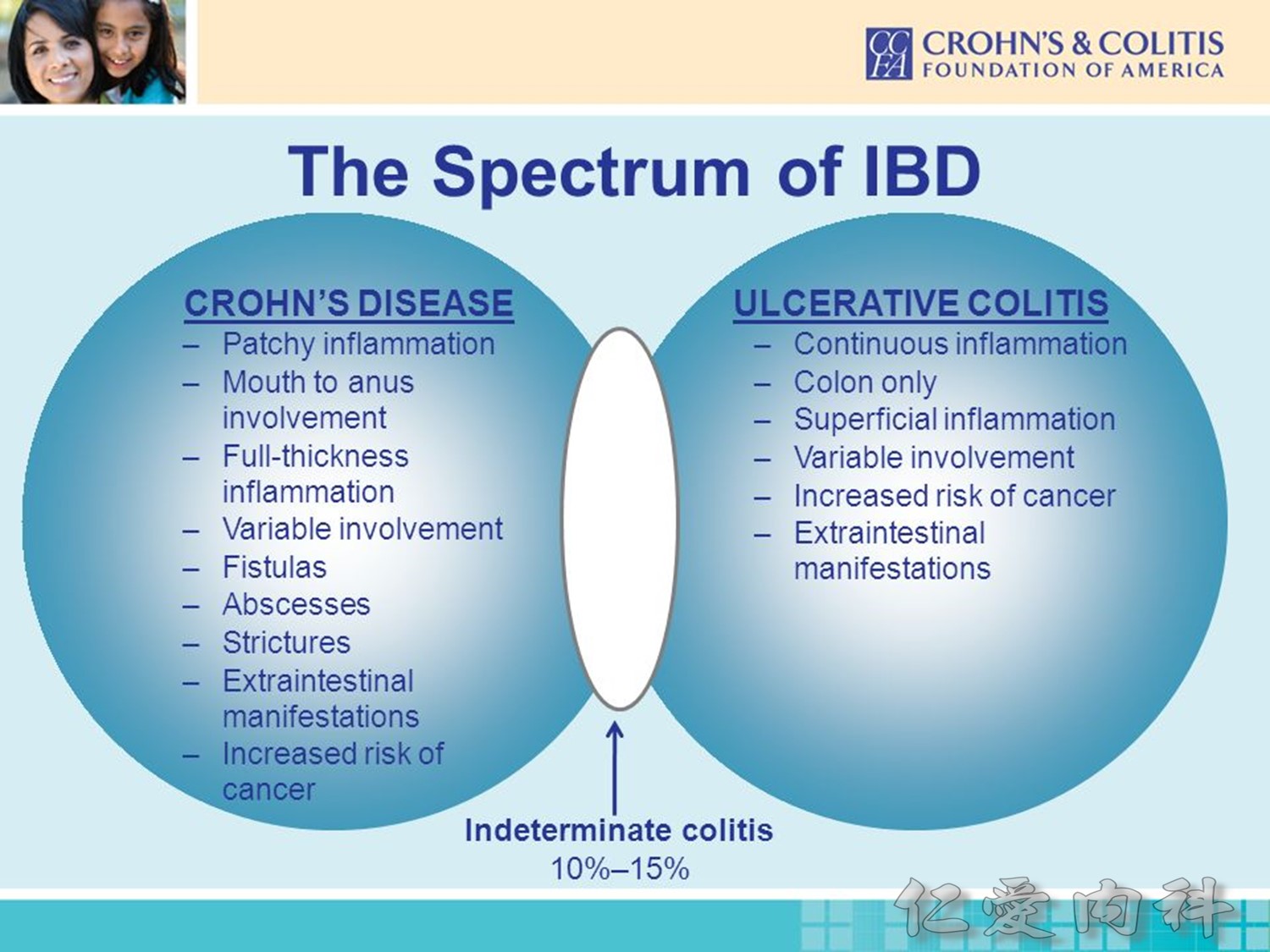
但是,臨床上還是有約 10-15% 的人無法區分是 UC 或是 CD。
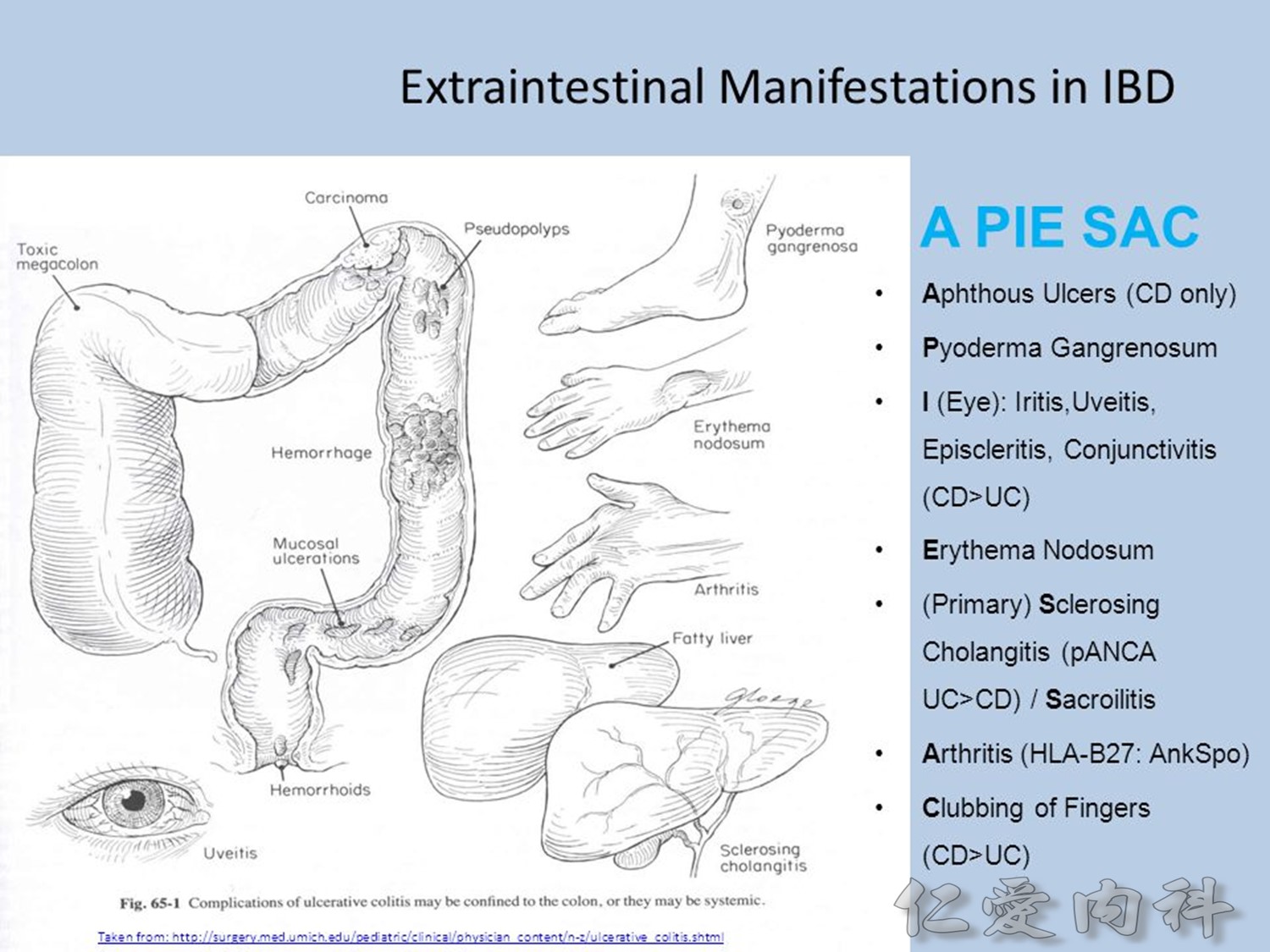
腸道外症狀 (extraintestinal manifestations) 有哪些? 可用口訣記誦:A PIE SAC:
- Aphthous ulcers (CD only)
- Pyoderma gangrenosum
- Iritis, uveitis, episcleritis (CD > UC)
- Erythema nodosum
- Sclerosing cholangitis (PSC: primary scolerosing cholangitis, pANCA, UC > CD)
- Arthritis (HLA-B27: ankylosing spondylitis [sacrolitis])
- Clubbing of fingertips (CD > UC)
腸道外症狀除了 PSC 在 UC 比較常見外,其他都是 CD 較常見。
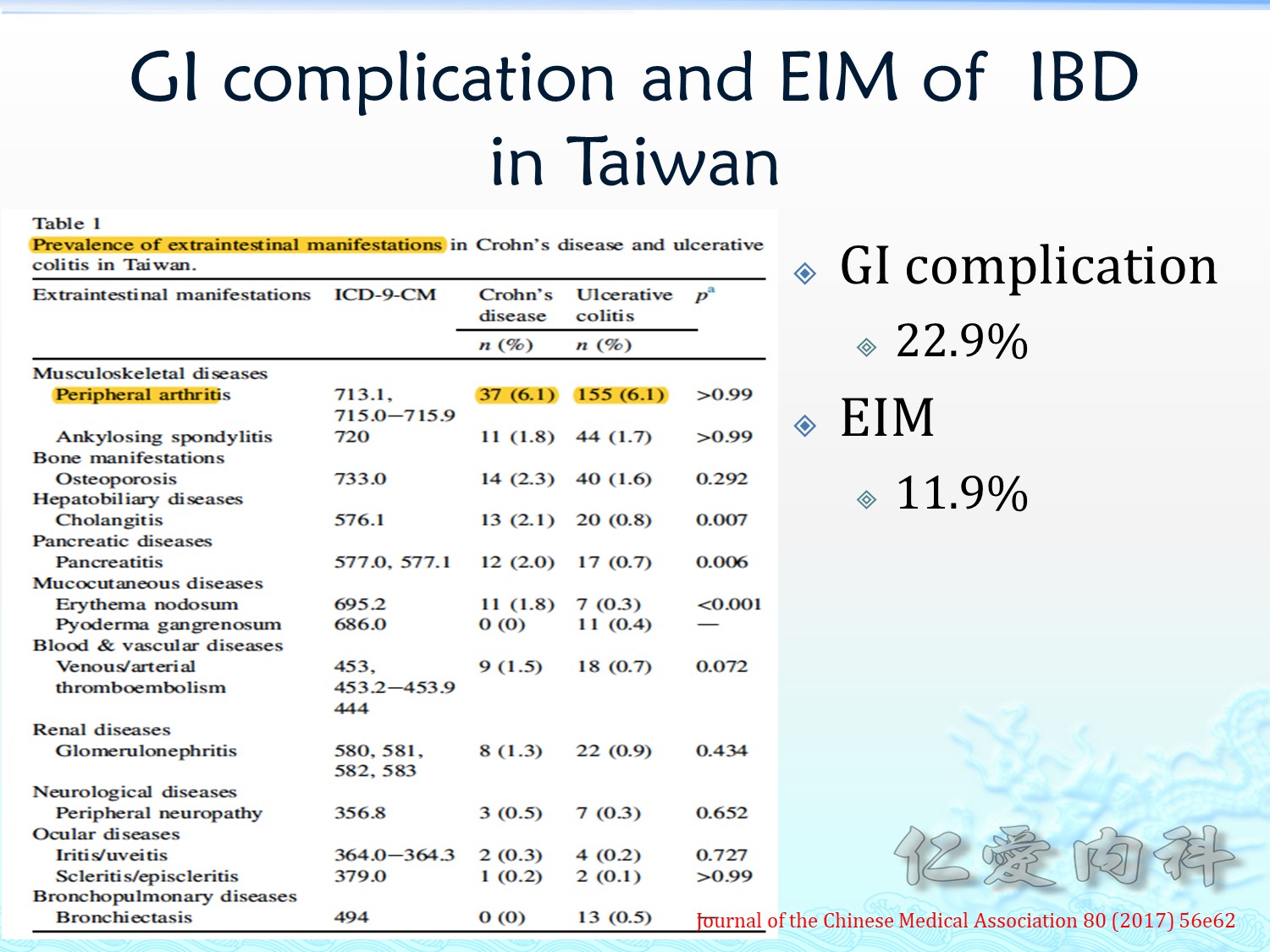
台灣的腸道外症狀不常見,約佔 11.9%,多是 arthritis。

壞疽性膿皮症 (pyoderma gangrenosum) 是一種罕見的自體免疫疾病 (無菌性嗜中性球發炎性皮膚病), 目前病因不明, 也稱為 phagedena geometrica, dermatitis gangrenosa 或 phagedenic pyoderma,常侵犯下肢脛骨前區為主, 會造成潰瘍性的皮膚病灶, 百分之五十與系統性疾病相關,例如發炎性腸病 (inflammatory bowel disease)、免疫相關性關節炎、 血液腫瘤疾病、 肝炎、 或後天免疫缺乏症候群 (AIDS) 等等。 其初始表現有時似感染性皮膚疾病, 如櫛、 膿皰、 毛囊炎、 蜂窩性組織炎、 或壞死性筋膜炎等, 但治療方式完全不同; 此病需給予免疫調節藥物及類固醇治療, 而非抗生素或手術清創。 [內科學誌 2012:23:137-143]
結節性紅斑 (erythema nodosum) 是一種脂膜炎 (panniculitis),通常以急性突發的疼痛對稱性紅腫來表現,好發於下肢的伸側 (extensor side)。結節性紅斑的病灶可以自行消退後又復發,但不會伴隨皮膚潰瘍、結疤或萎縮的情形。雖然以皮膚的症狀來表現,但一般認為它是由某種其他身體疾病或狀態所誘發的一種過敏反應 (hypersensitivity),最常見的誘發因子如:感染 (如 A 型鏈球菌咽喉炎之後)、 類肉瘤症 (sarcoidosis)、風濕免疫疾病、發炎性腸道疾病 (inflammatory bowel disease)、藥物 (磺胺類藥物及避孕藥最常見)、懷孕或惡性疾病等。[內科學誌 2015:26:313-318]
Diagnostic Studies

目前沒有一個好的實驗室方法能有效區分 UC 與 CD。
約 65% 的 UC 病人會有 perinuclear Antineutrophil cytoplasmic antibodies (pANCA);約 60-70% 的 CD 患者會有 antibodies to Saccharomyces cerevisiae (ASCA)。(Saccharomyces cerevisiae is a species of yeast.)
Fecal calprotectin 可在任何的發炎狀況升高,但是如果 fecal calprotetin 為 negative,應可排除 IBD 的可能。
若病人有可能有 intestinal stricture(s),膠囊內視鏡的檢查要小心使用。
IBD 要與 intestinal tuberculosis, Behçet’s disease, 以及其他可以導致腸道發炎的狀況進行鑑別診斷。
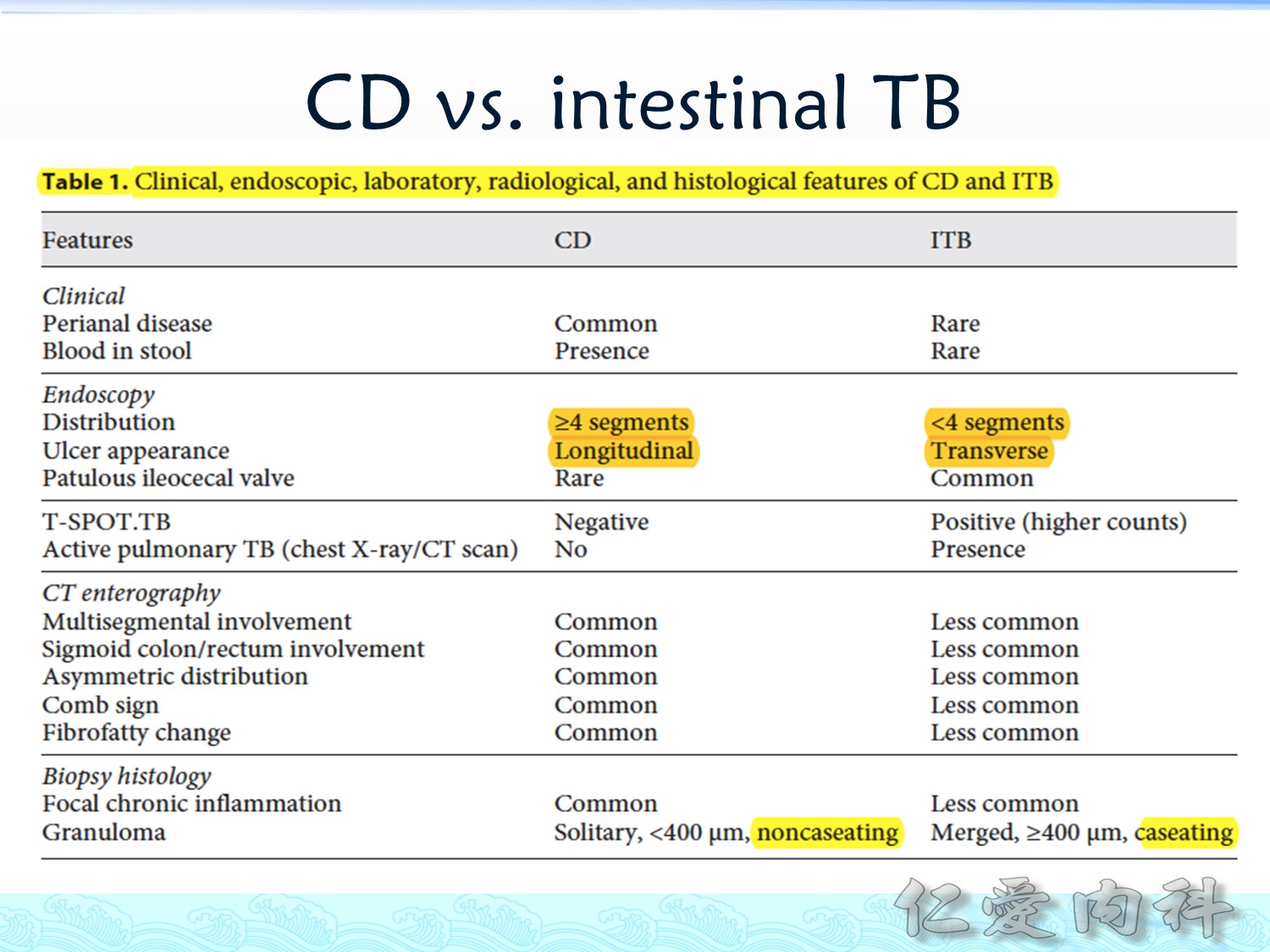
Intestinal tuberculsis 與 CD 的差異在於:CD 的 ulcer 為 longitudinal 且多於 4 個 segments,TB 多為 transverse 且侵犯少於4個 segments;TB 的 IGRA 為 positive;TB 不常出現如 CD 常見的如 cobblestone appearance 的 pictures; granumola 的組織學上表現 CD 為 noncaseating/noncaseous, TB 則為 caseating/caseous。
Therapeutic Approach & Management


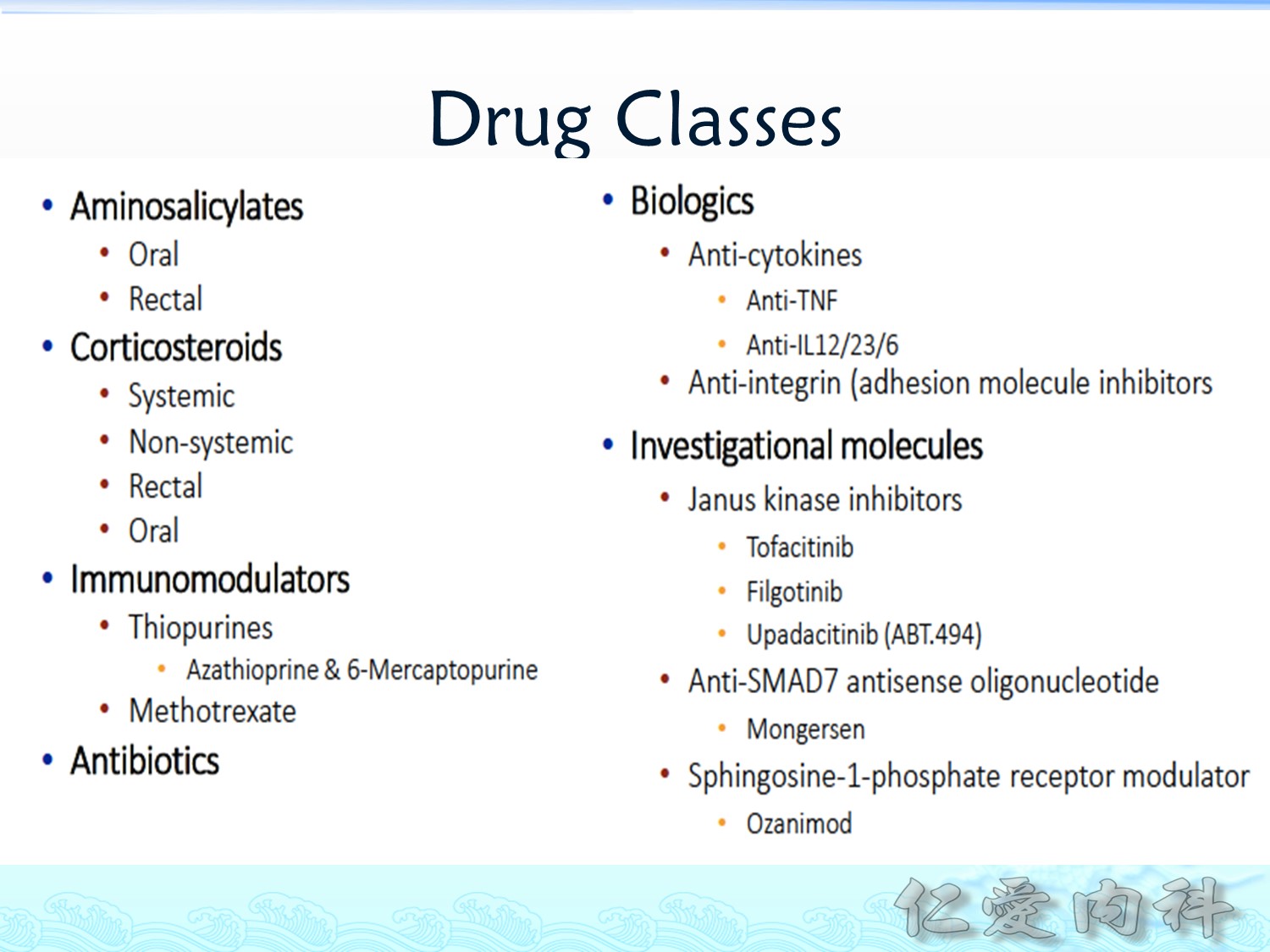
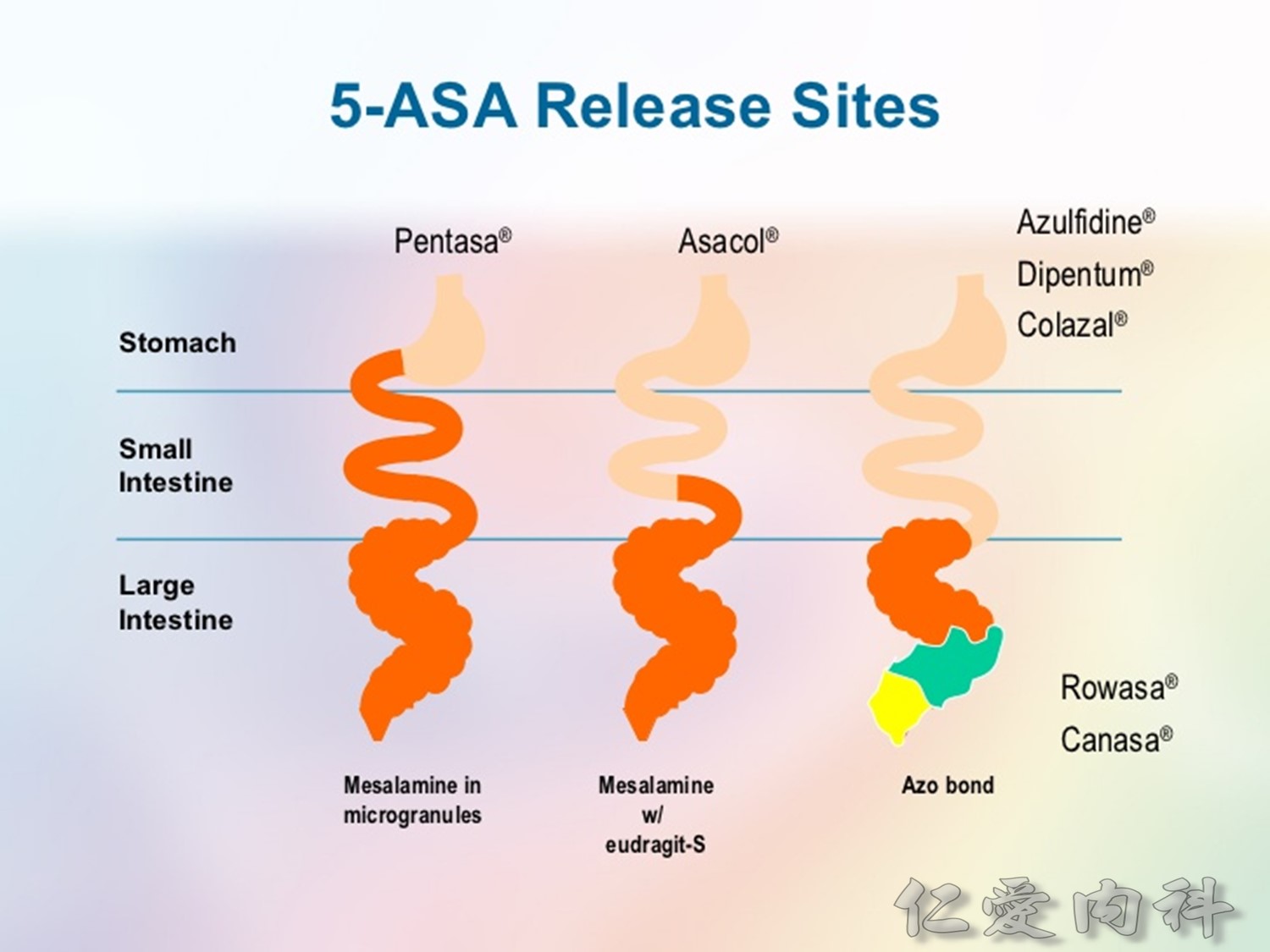
不同的 5-ASA 製劑可以治療不同段的腸道疾病。
Budesonide MMX (a gut-specific corticosteroid) 的系統性副作用較少,但是台灣沒有。
Corticosteroids 的重要副作用有 osteoporosis, hypertension, growth retardation, hyperglycemia, cataracts…
使用 corticosteroid 超過 3 個月者應接受 bone densitometry 的檢查,適時檢查 vitamin D levels 並且給予最大必要之補充,儘快使用 steroid-sparing agents 來 taper corticosteroids.
Immunomodulators 有三種—6-Mercaptopurine (6-MP), Azathioprine, Methotrexate (MTX)—小心 bone marrow suppression,與長期使用所增加的 lymphoma risk。

Antibiotics 常用的有 metronidazole, ciprofloxain, rifaximin
Fecal Microbiota Transplant (FMT)、Probiotics & Prebiotics、Omega-3 Fatty Acids 也是治療手段。
Biologic therapy 可以在前述治療方法都無明顯效果或需長期使用前述副作用較大之治療方法時使用,或者在 CD 病人有 fistula 或預防其術後 CD 的在發生時使用。
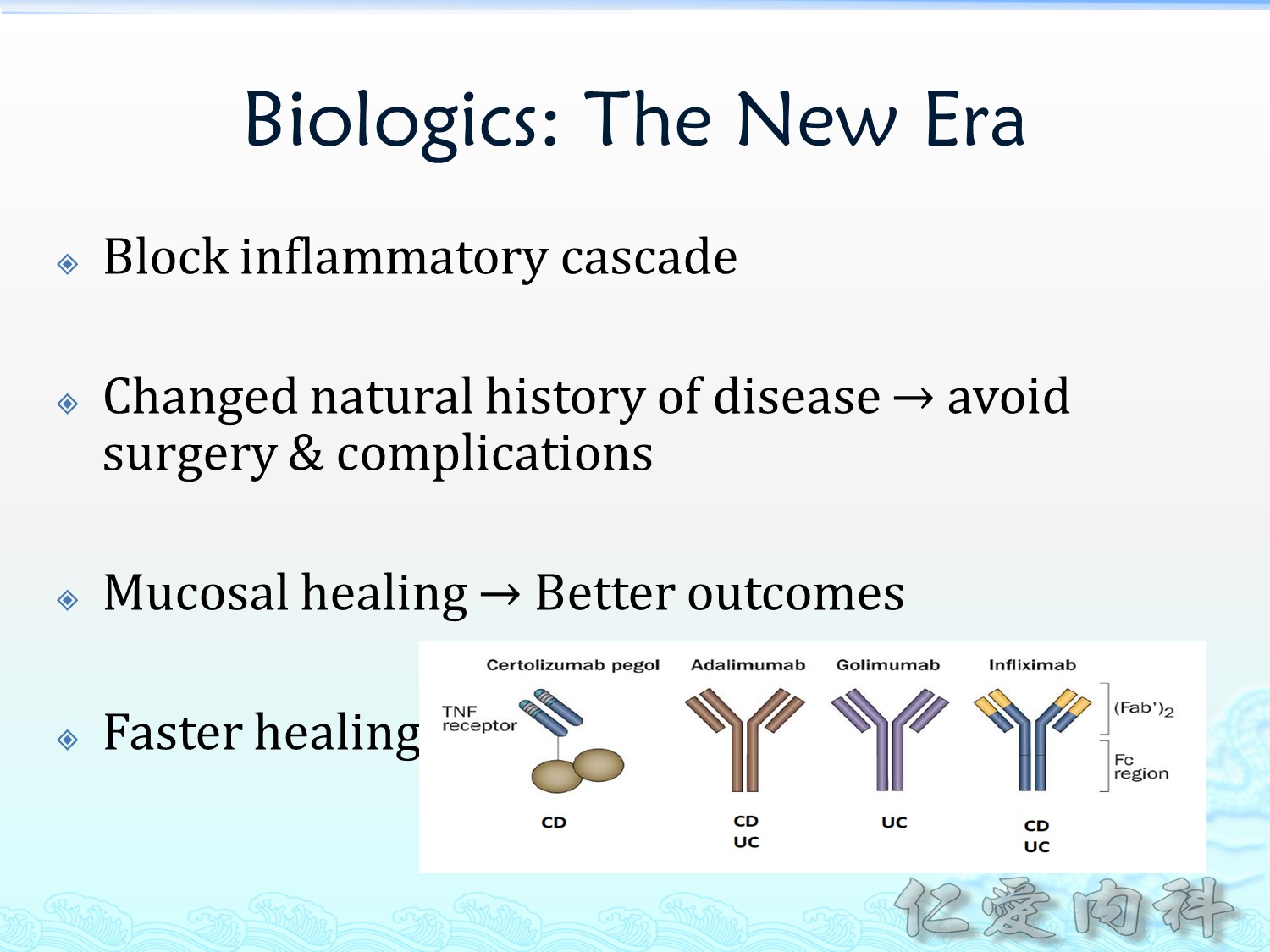
使用 anti-TNF agent (e.g. adalimumab [例如Humira]、infliximab [例如 Remicade]、golimumab [例如 Simponi]、vedolizumab [例如 Entyvio]) 前應該要先檢查病人是否有 tuberculosis 或 HBV。
也可以 combine 其他治療方式/藥物來達成更好的效果。
UC 會增加 colorectal cancer 的風險,約 25% 的患者建議需要接受 total proctocolectomy,特別 (surgical indications) 是 severe hemorrhage, perforation, fulminant colitis, toxic megacolon, medical failure 等狀況出現時。
原則上 right-sided UC 診斷 8 年以上的患者應該接受定期 colon cancer 篩檢,left-sided UC 診斷 12 年以上的患者應該接受定期 colon cancer 篩檢。
Patients should receive an initial screening colonoscopy eight years after the onset of pancolitis and 12 to 15 years after the onset of left-sided disease; follow-up colonoscopy should be repeated every two to three years.
Am Fam Physician. 2007 Nov 1;76(9):1323-1330

CD 患者何時接受手術? Strictures causing obstructive symptoms, Intra-abdominal abscess, fistulas or perianal disease refractory to medical therapy.
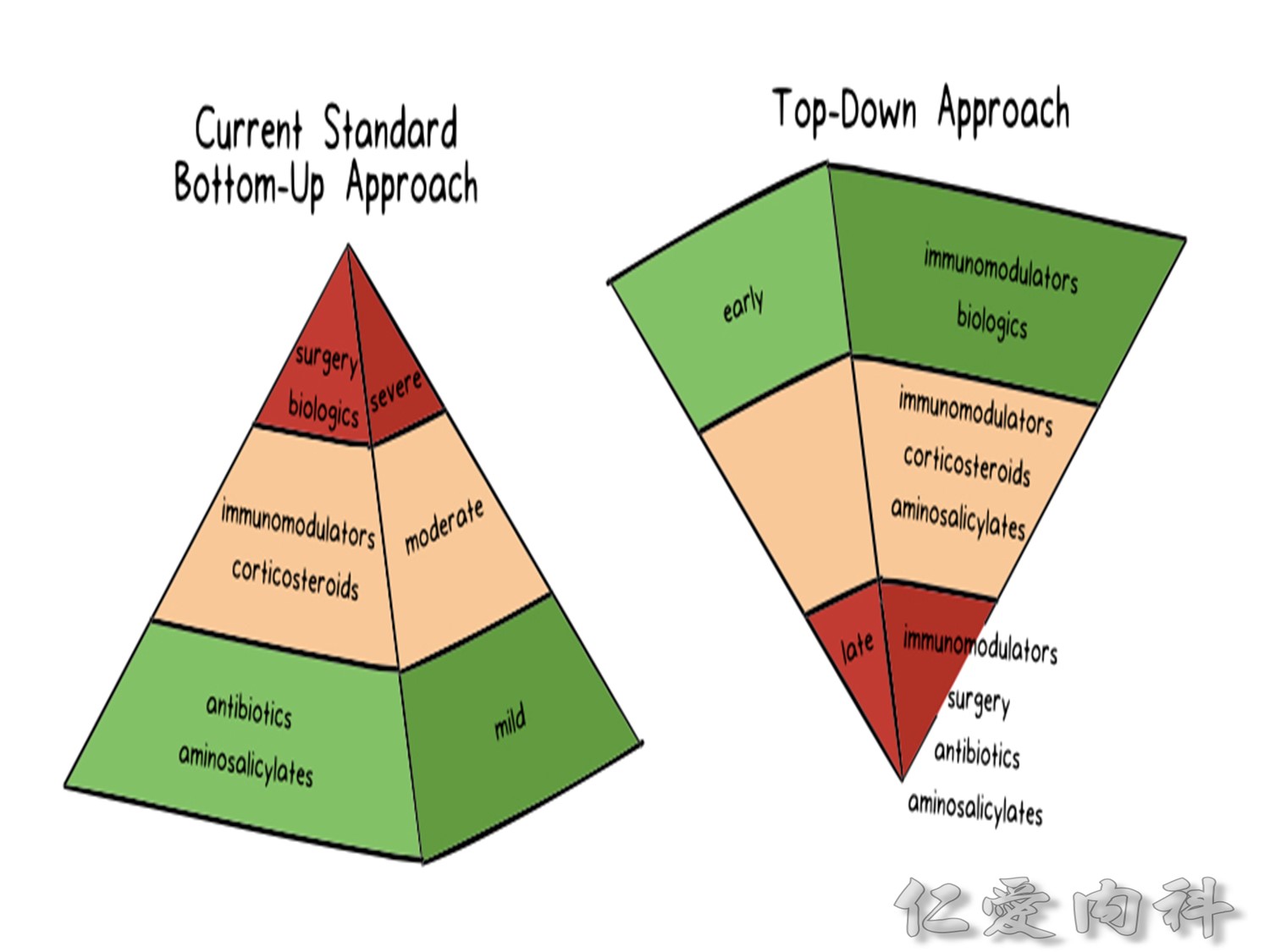
目前的 standard therapy approach 還是 bottom-up approach。
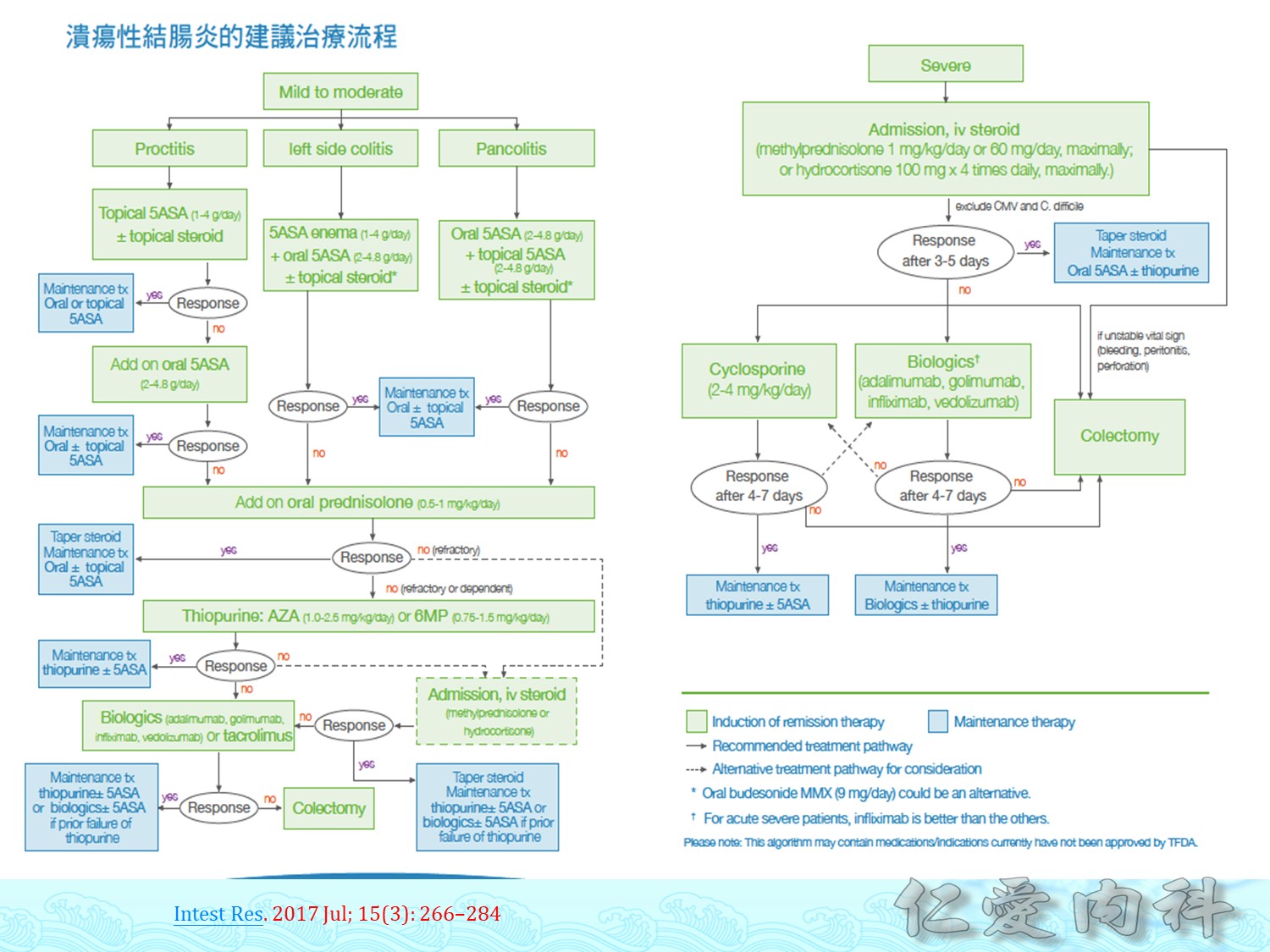
類固醇在所有的 IBD 都不能當成一個 maintenance 的治療,需要儘早 tapering with the use of additional steroid-sparing therapies。
When deciding to initiate a 5-ASA, check the patient’s glomerular filtration rate and what other drugs the patient is using.
When deciding to initiate anti-TNF therapies, keep in mide the higher rates of infection. Patients with advanced heart failure also should not be treated with anti-TNF therapies. Those on anti-TNF therapies should not receive live vaccines (e.g. zoster vaccine).
With regard to thiopurines (e.g. 6-mercaptopurine and azathioprine), keep in mind the increased risk for lymphoma (& lymphoproliferative disorder) and skin cancer over time, and be sure to check potential drug interactions.
Regarding the use of methotrexate, monitoring liver function and checking drug interactions are necessary.
Vedolizumab (an anti-integrin agent) is indicated for both CD and UC.
長期 IBD 疾病的進展本身就會增加患者的 infection 的風險,也會導致 anemia, malnutrition, 與 dehydration,這些都必須以藥物治療 IBD 來緩解,但是這些又與藥物造成的副作用難以區分。
IBD 的患者應接受 pneumococcal polysaccharide vaccine 23-valent 與 pneumococcal conjugate vaccine 13-valent。
Harrison 的表格
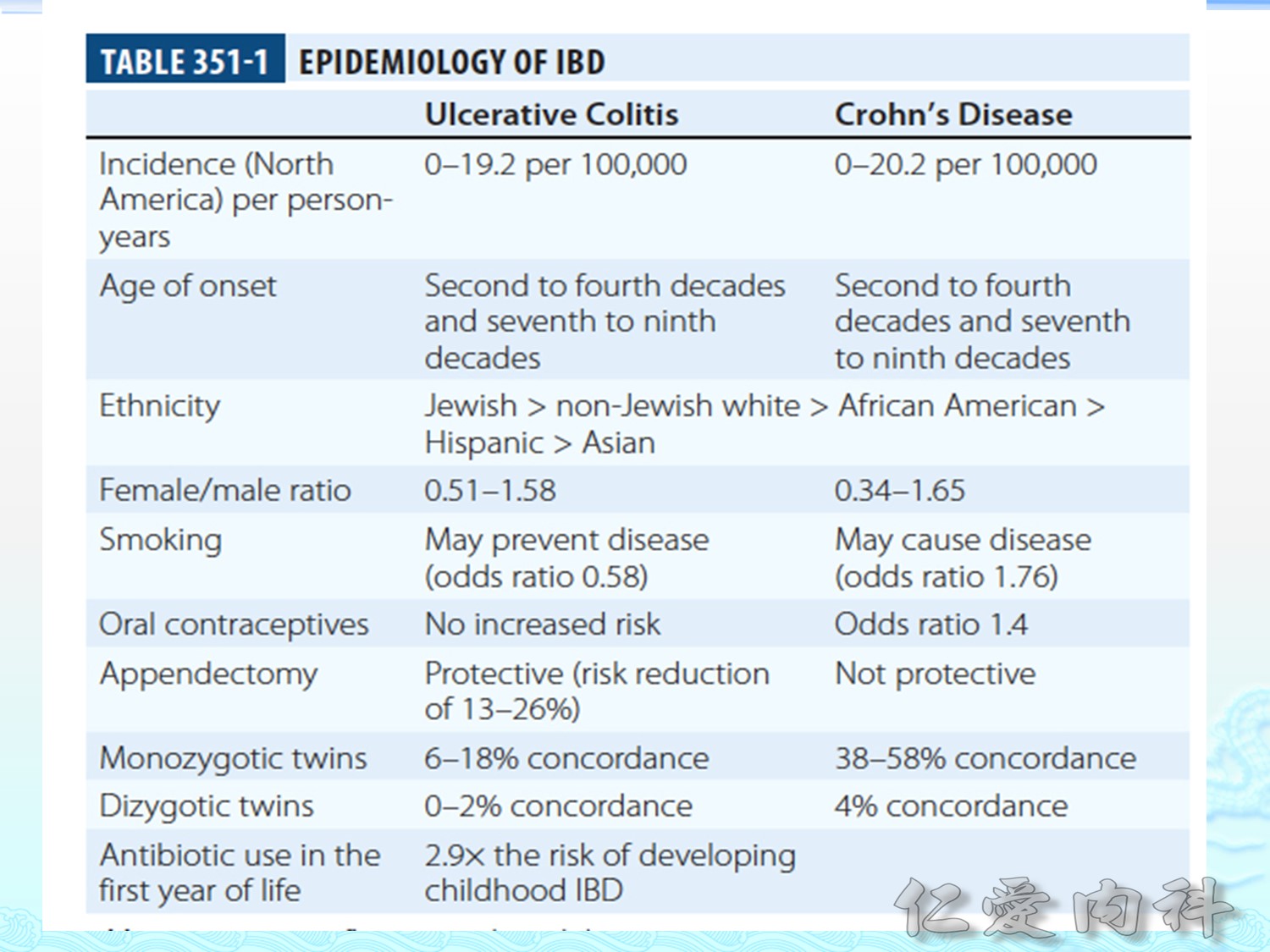
Smoking 可減少發生 UC 的風險,但是會增加發生 CD 的風險。
Oral contraceptives 對 UC 的發生風險沒有影響,但是會增加發生 CD 的風險。
Appendectomy 會降低 UC 的發生風險,但是不會改變發生 CD 的風險。
但是很多原因機轉不清楚。
[comment: 好的都沒有 CD 的份]
另外,個人的出生方式會影響個人日後發生IBD的風險,NSD 較 CS 發生 IBD 的風險低;breasting feeding 也會降低 IBD 的風險。