作者/講者: 張詔程 醫師
指導者: 王喬弘 醫師
整理: Ian YC Chen, MD
校稿: Ian YC Chen, MD
上次校閱: 2018/04/05
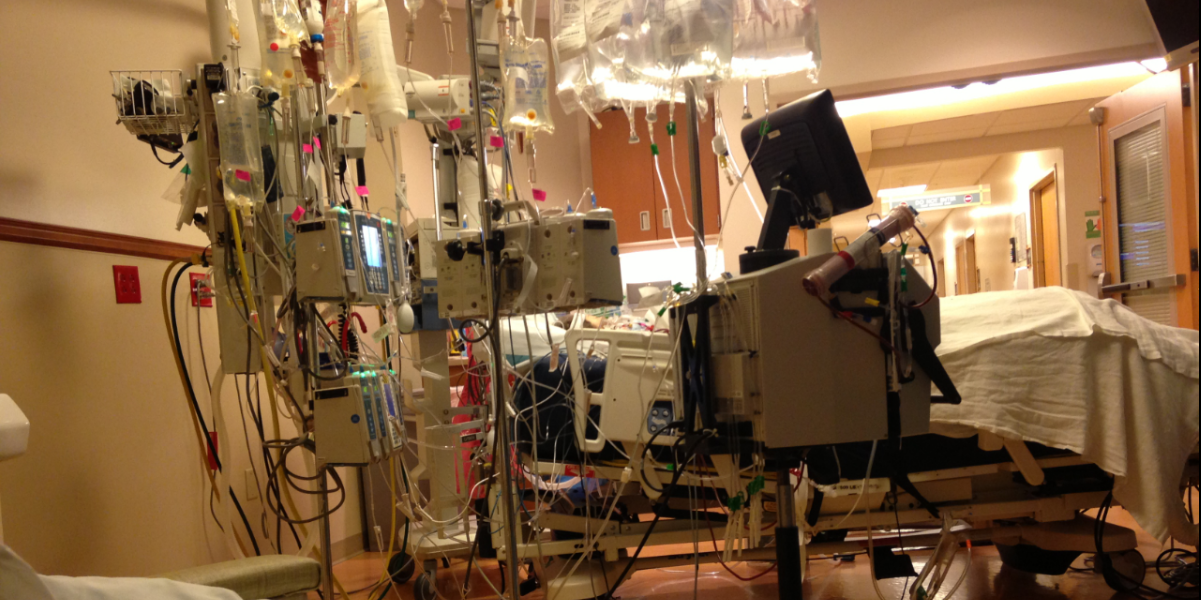
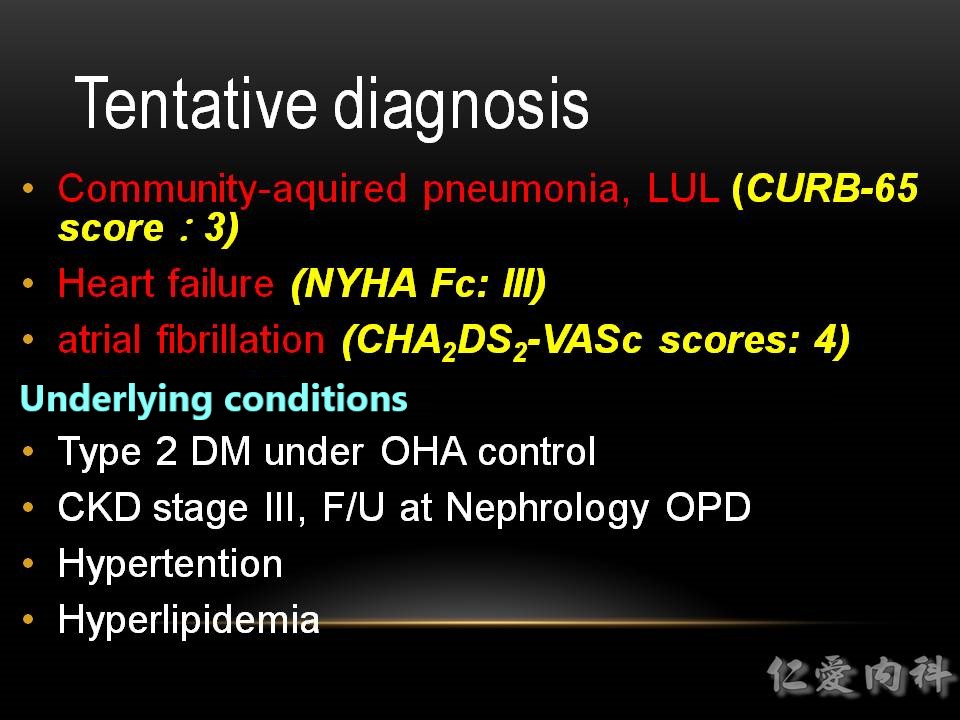
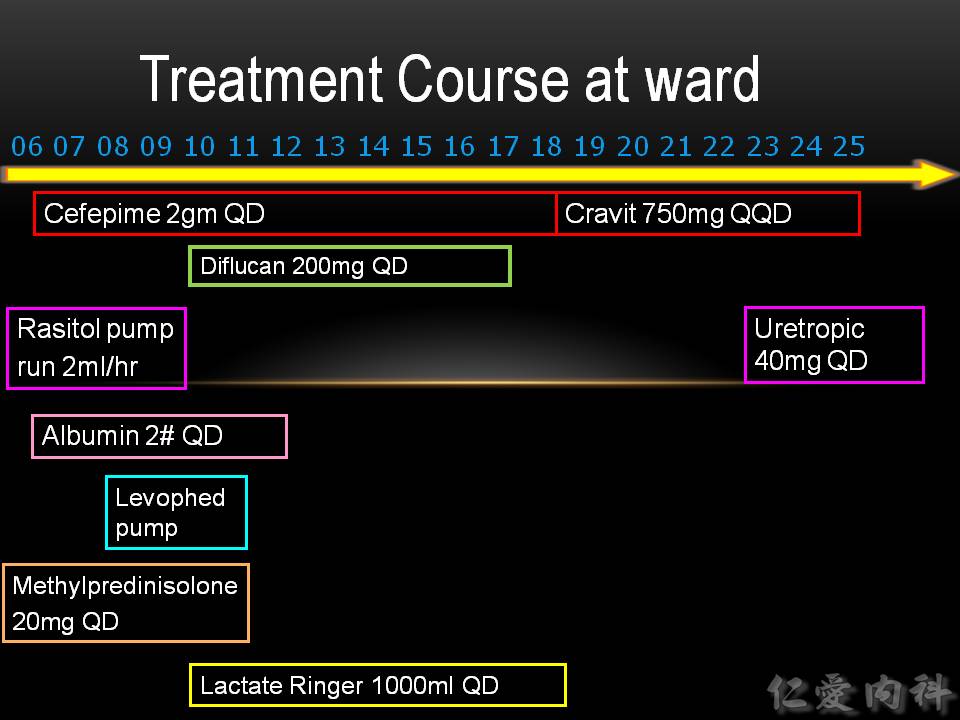
Case Scenario:
This is an 82-year-old retaired man admitted from the OPD becasue of progressive, intermittent shortness of breath, which is the worst during the past 3 to 4 days. He lives alone and is able to take care of himself wihout difficulties.

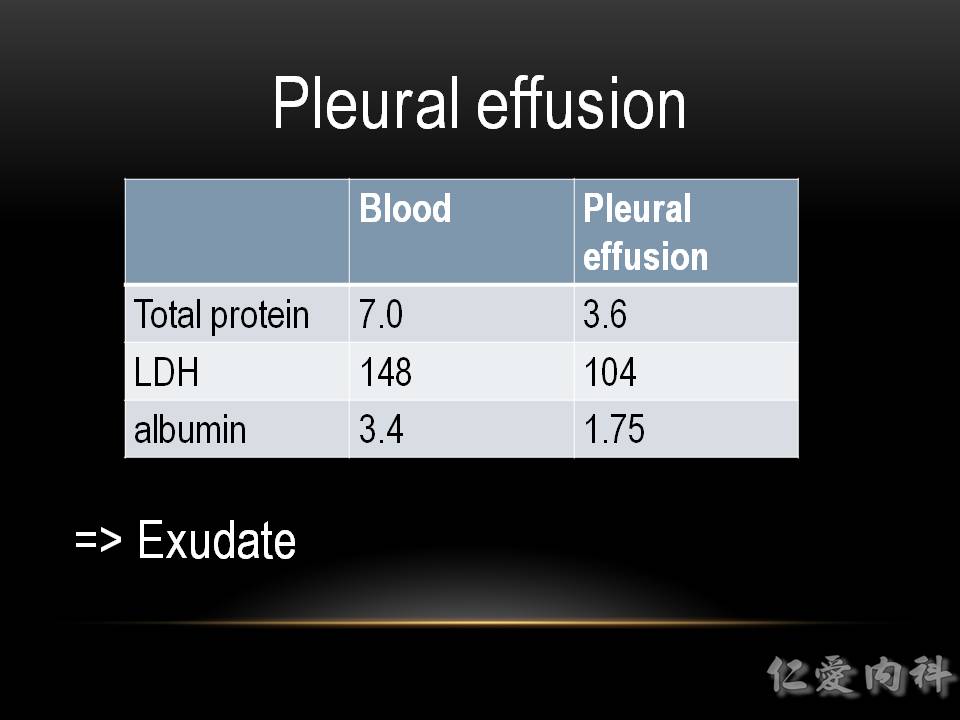
Pleural effusion analysis by Light’s criteria:
三個符合一個, 則有相當高的機會是漏出液(Exudate), 都不符合則極有可能是滲出液(Transudate)
a. 肋膜積水/血清蛋白質比值>0.5
b. 肋膜積水/血清LDH比值>0.6
c. 肋膜積水LDH濃度>血清上限值的2/3 (在Light當年的研究, 這個上限值的2/3是200 IU/L)
有一部分的 exudate其實應是 transudate (例如被打過利尿劑的heart failure related transudate), 稱為 pseudo-exudate。
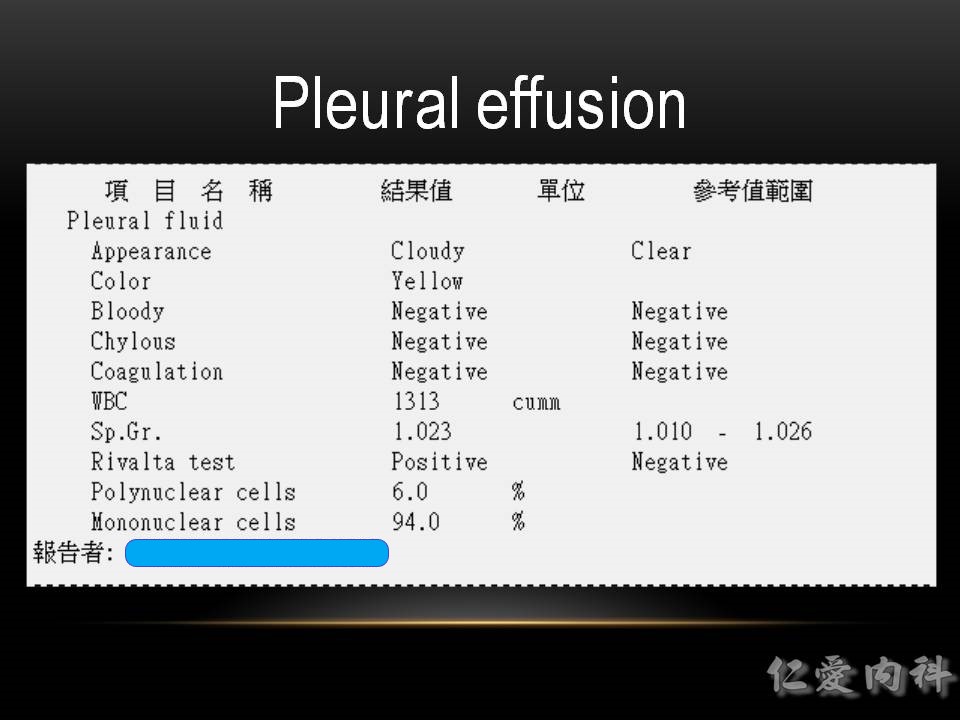
Exudate表示為發炎性反應造成之 pleural effusion。
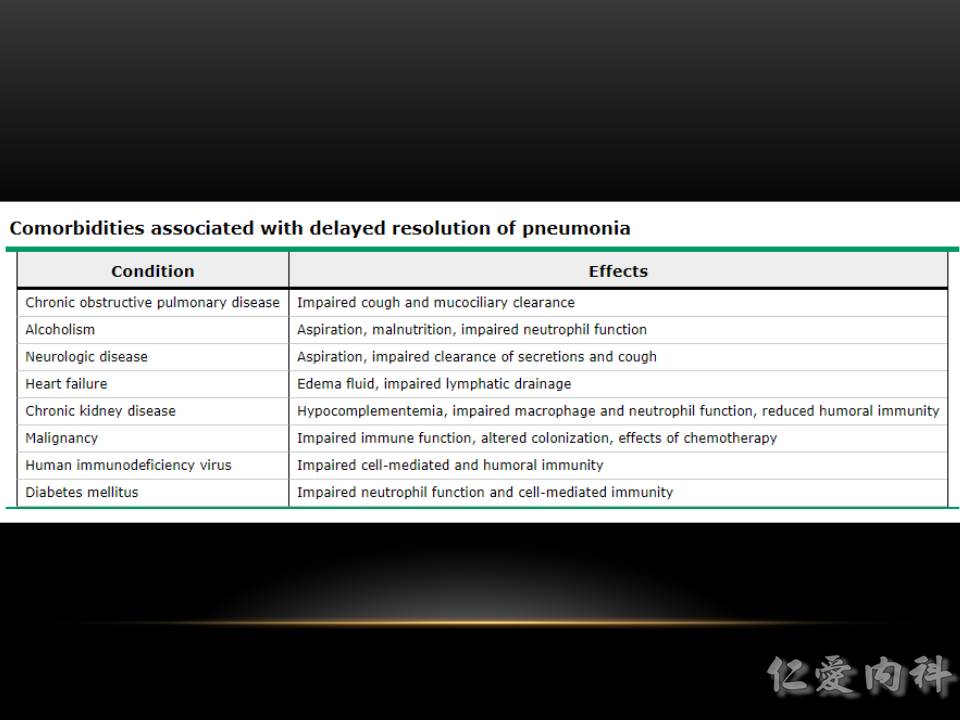
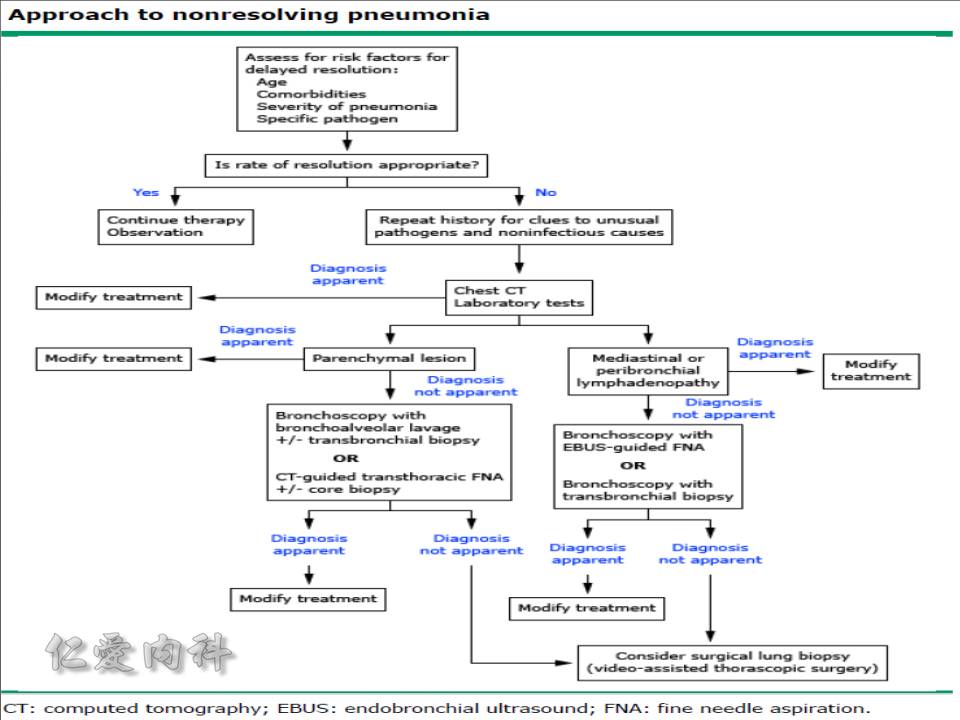
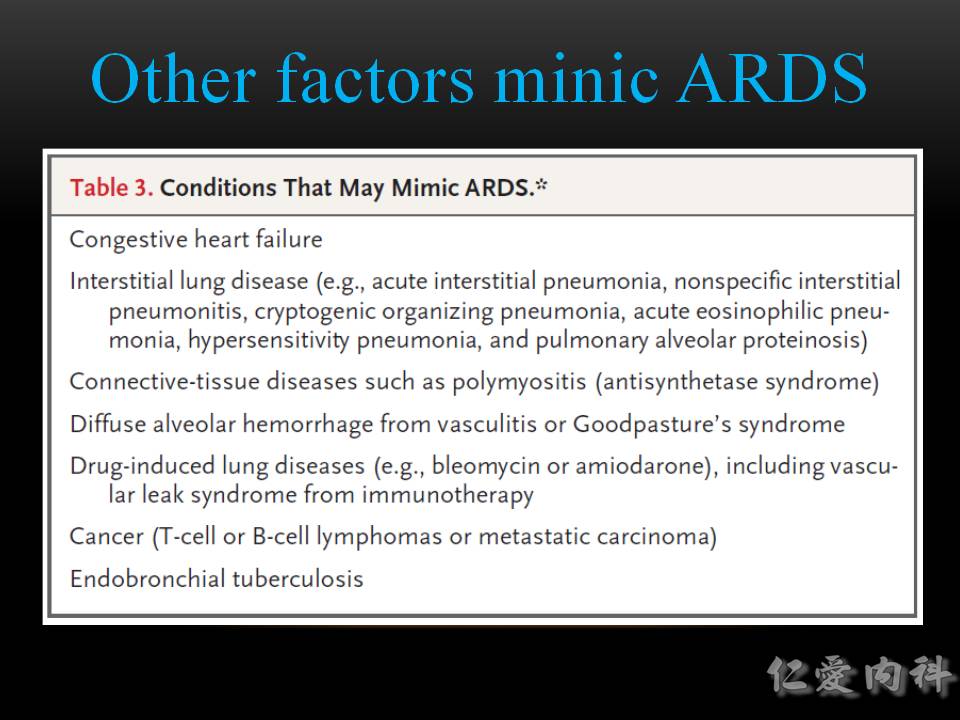
對於一開始的 bacterial pneumonia 診斷有懷疑時, 加上一段時間的 (經驗性或是培養證實有效的) 抗生素治療成效不佳時, 應該要開始懷疑其他可能之原因: COPD, heart failure complicated with pulmonary edema, malignancy, pulmonary hemorrhage, connective tissue diseases。
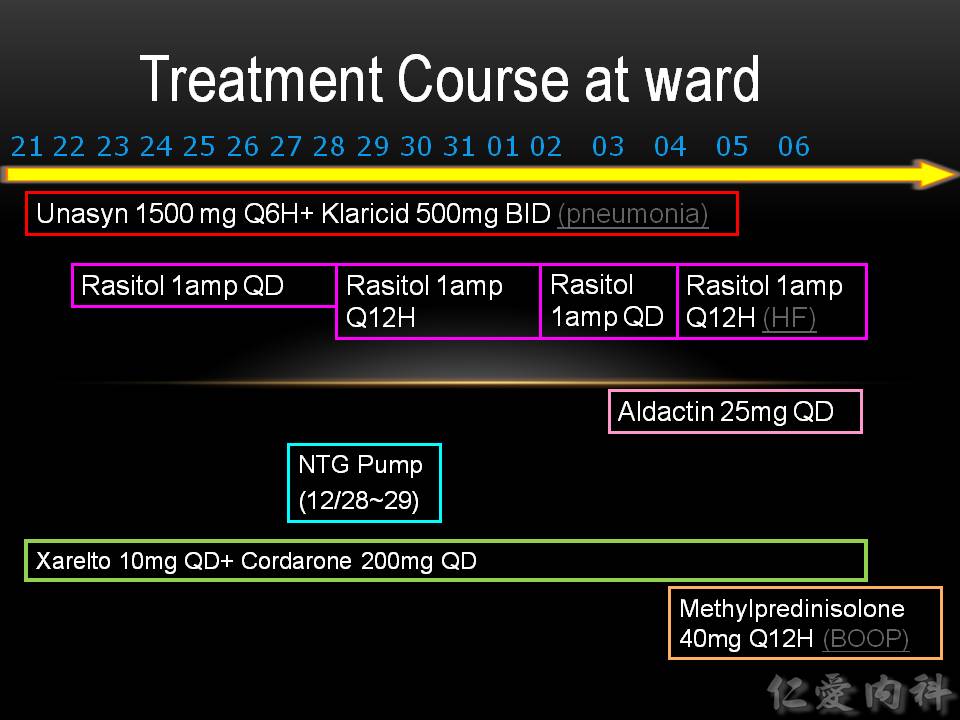
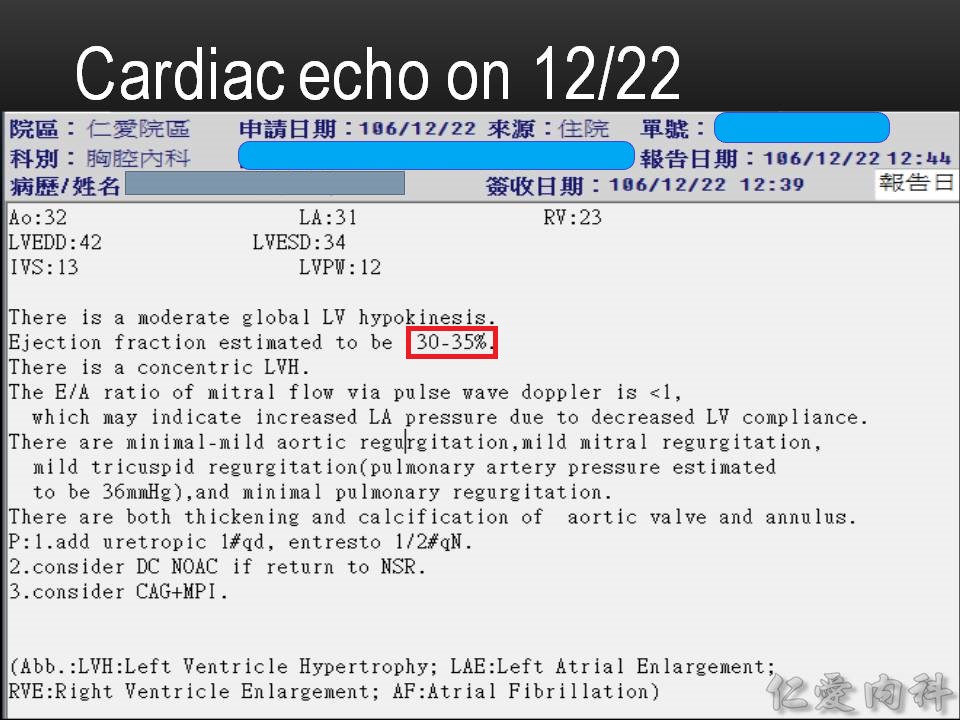
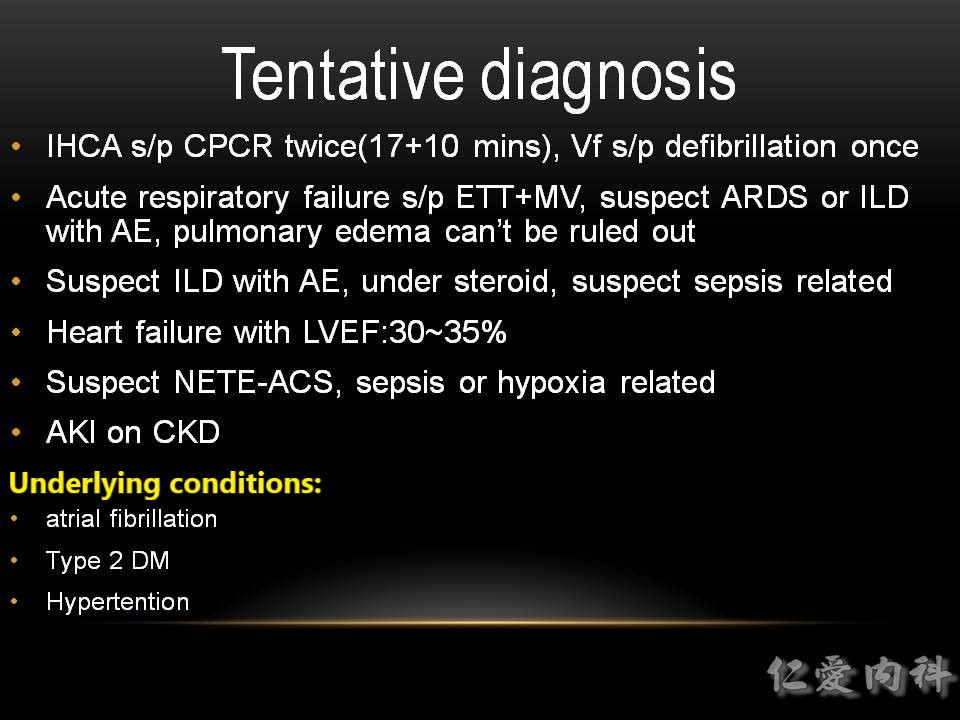
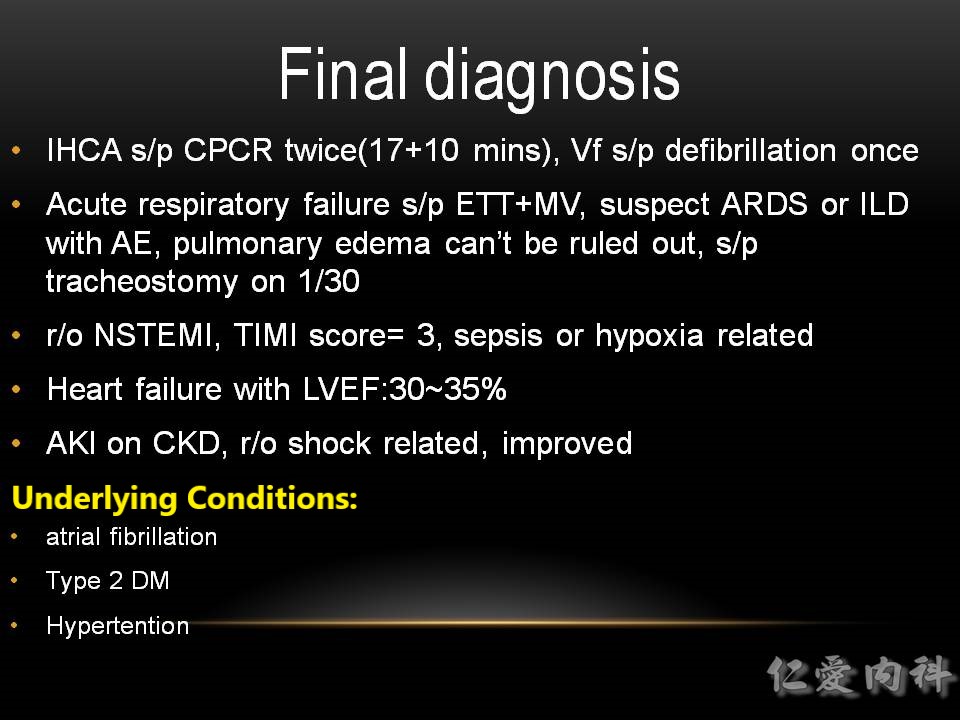
Heart failure with reduced EF is established.
病人已經有atrial fibrillation, 推測心臟結構上應該已經長年異常, 因此針對病人的 heart function restoration的可能性, PCI在目前而言應該沒有幫助, 此階段應積極治療 hear failure 與不敢輕易排除的 bacterial pneumonia (or whatever pulmonary inflammatory process)才是當務之急。
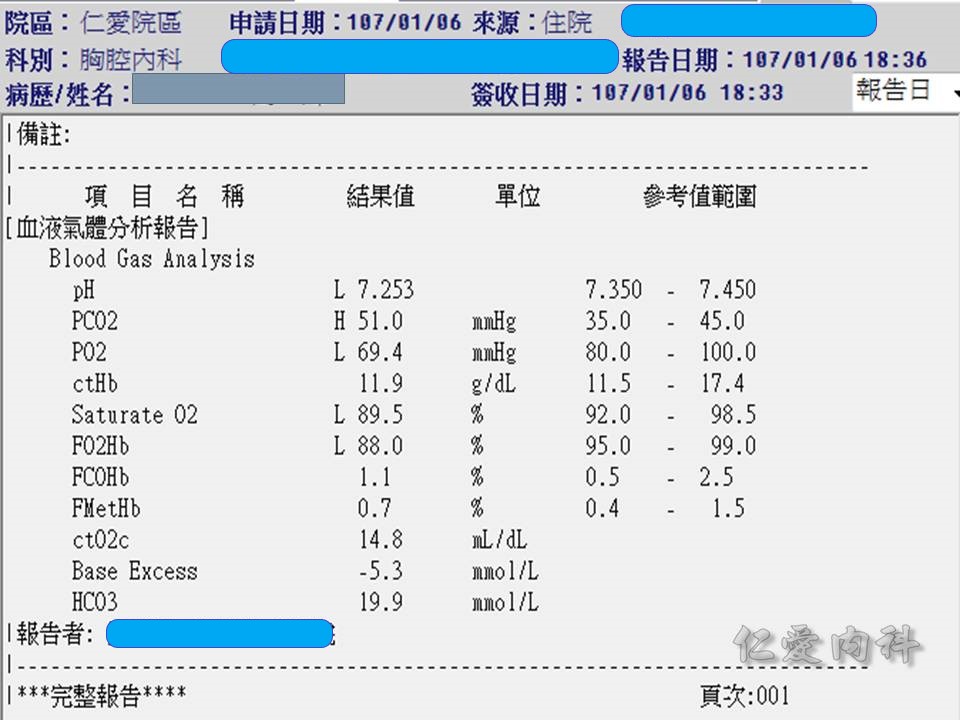
此時的 calculated PaO2/FiO2 ratio 已經不及100, 若不是 decompensated heart failure, 就應該考慮ARDS。
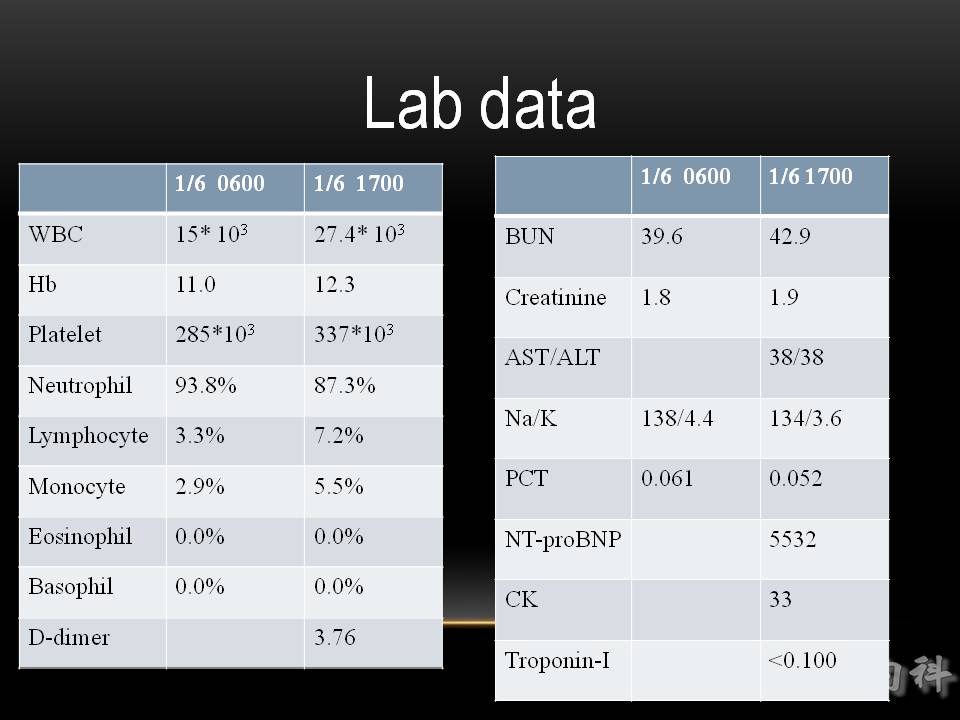
若是 decompensated heart failure (也許能從physical examination得到一些 clues, e.g., JVE, S3 or S4, new murmur [acute MR], rales, hepatojugular reflux and so on; 切記, lab 的 NT-ProBNP需要等一段時間, 恐怕延誤治療), 務必記得要立刻追查原因 (e.g., AMI? severe hypertension? rupture of a cardiac valve? fluid over load with an undiscovered acute renal failure?)
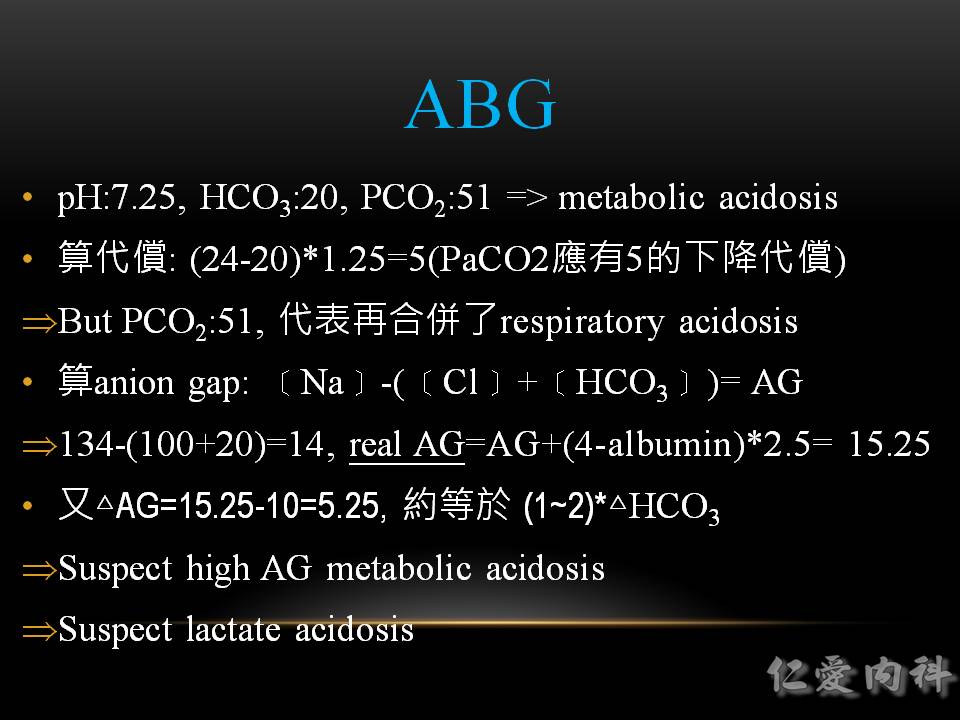
當然, metabolic acidosis的原因相當多, 一般的口訣記憶可用 “MUDPILERS”
- Methanol
- Uremia
- DKA/Alcoholic KA
- Paradehyde
- Isoniazid
- Lactic acidosis
- EtOH/Ethylene glycol
- Rhabdo/Renal failure
- Salicylates
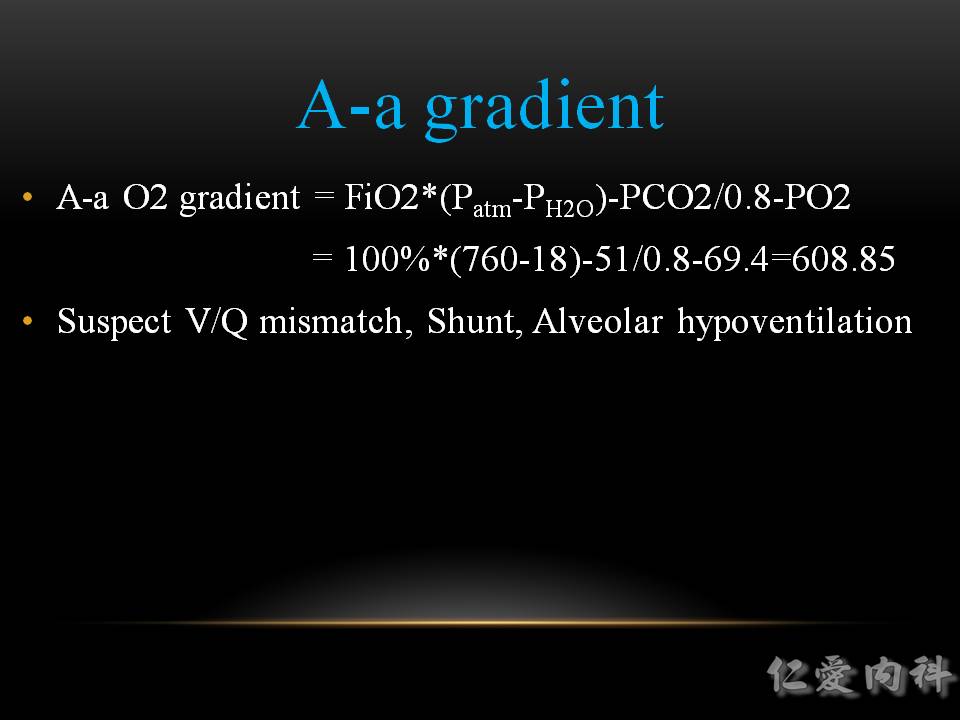
這裡的 A-a oxygen gradient 計算有些錯誤(sea level 的 partial pressure of H2O 應是 47), 但數值偏高是可確定的。
正常的數值約是 (Age/4) + 4
| Causes of Hypoxemia | A-a O2 Gradient Shift | |
|---|---|---|
| 1 | V/Q Mismatch (ex: PNA, CHF, PE, ARDS, atelectasis, etc) | Elevation |
| 2 | Shunt (ex: PFO, ASD, pulmonary AVMs) | Elevation |
| 3 | Alveolar Hypoventilation (ex: interstitial lung dz, environmental lung dz, PCP PNA) | Elevation |
| 4 | Hypoventilation (ex: COPD, CNS d/o, neuromuscular dz, etc) | Depression |
| 5 | Low FiO2 (ex: high altitude) | Depression |

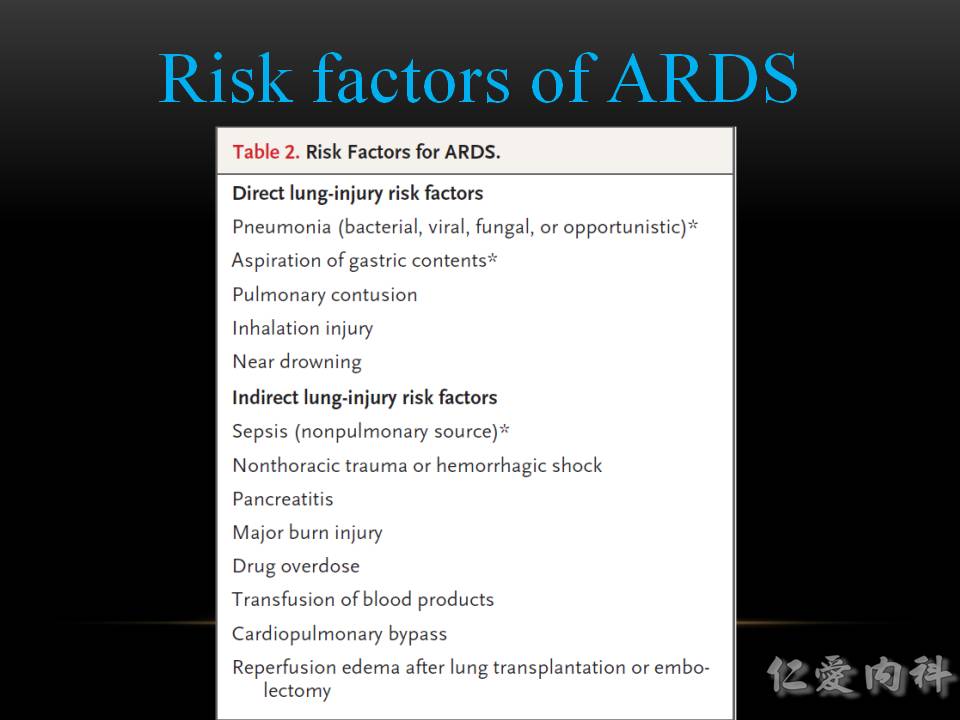
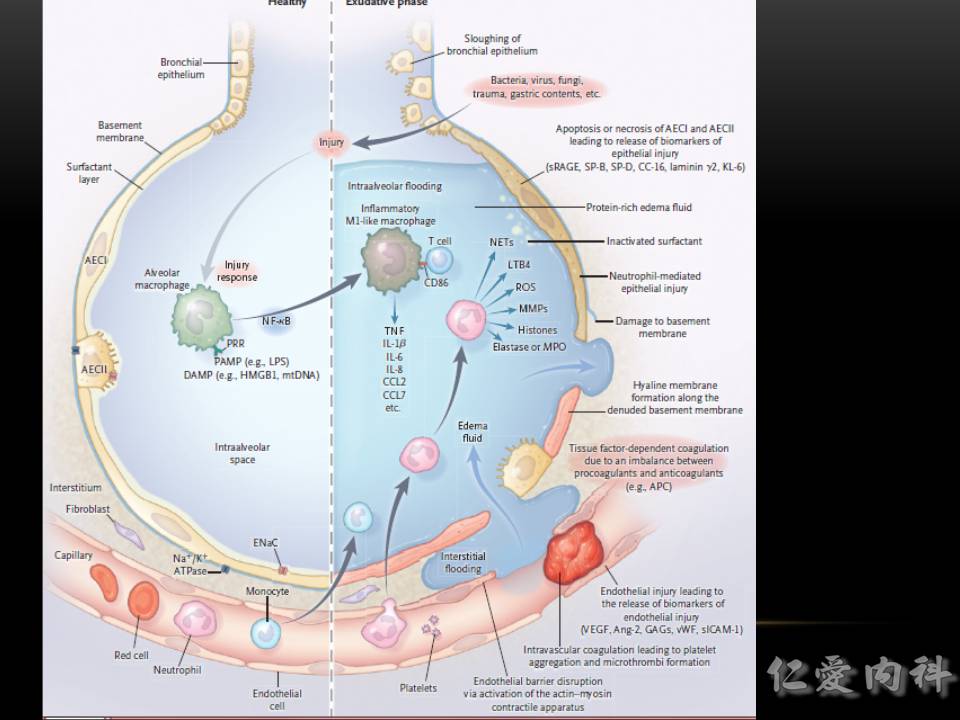
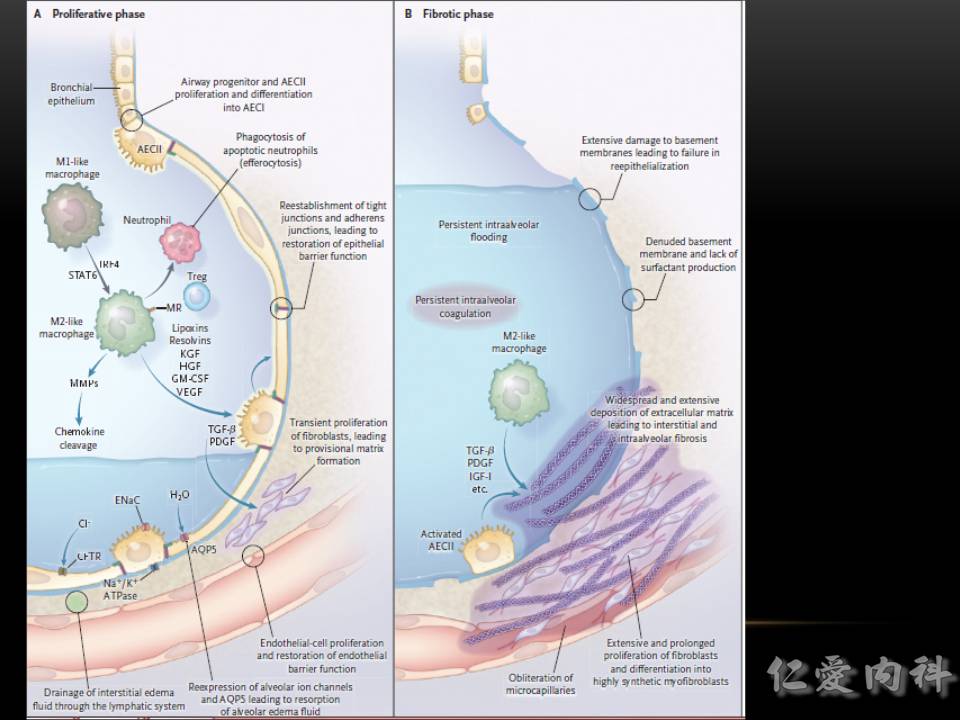
導致 ARDS 的原因可以用口訣記憶
A: Aspiration, Acute pancreatitis, Air/Amniotic embolism,
R: Radiation, TRALI
D: Drug overdose, DIC, Drowning, Diffuse lung disease
S: Sepsis, Shock, Smoke inhalation, Severe body injury (e.g., burn, trauma, multiple fracture, lung contusion)
✎ Pneumonia (~40%) > Sepsis (~25%) > Aspiration (~15%)
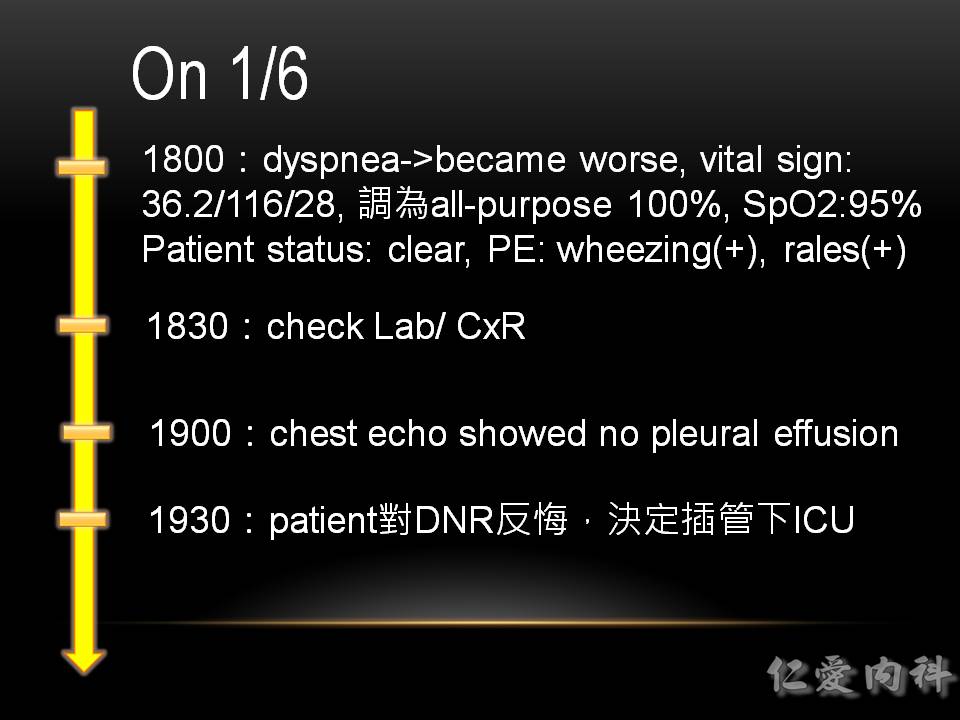
Heart (ejection fraction) 不好的病人, 容易 sudden death, 插管期間 desaturation 的 duration 應盡力縮短。
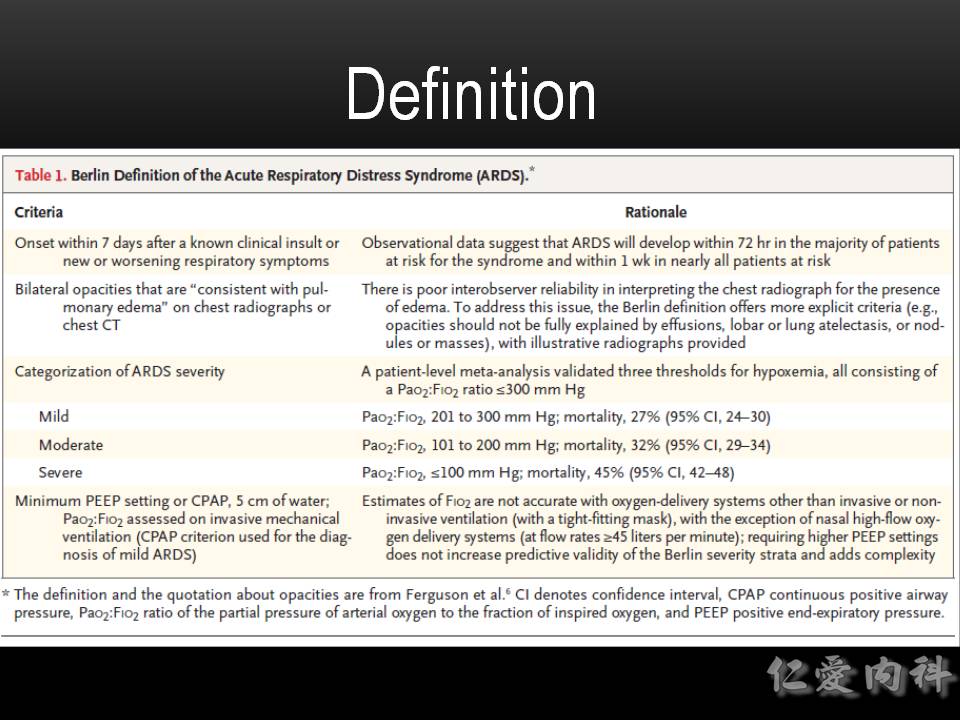
Acute Respiratory Distress Syndrome的定義可採用Berlin Definition (2011):
The acute respiratory distress syndrome (ARDS) was defined in 1994 by the American-European Consensus Conference (AECC); since then, issues regarding the reliability and validity of this definition have emerged. Using a consensus process, a panel of experts convened in 2011 (an initiative of the European Society of Intensive Care Medicine endorsed by the American Thoracic Society and the Society of Critical Care Medicine) developed the Berlin Definition, focusing on feasibility, reliability, validity, and objective evaluation of its performance. A draft definition proposed 3 mutually exclusive categories of ARDS based on degree of hypoxemia:
mild (200 mm Hg < PaO2/FIO2 ≤ 300 mm Hg),
moderate (100 mm Hg < PaO2/FIO2 ≤ 200 mm Hg), and
severe (PaO2/FIO2 ≤ 100 mm Hg)
and 4 ancillary variables for severe ARDS: radiographic severity, respiratory system compliance (≤40 mL/cm H2O), positive end-expiratory pressure (≥10 cm H2O), and corrected expired volume per minute (≥10 L/min). The draft Berlin Definition was empirically evaluated using patient-level meta-analysis of 4188 patients with ARDS from 4 multicenter clinical data sets and 269 patients with ARDS from 3 single-center data sets containing physiologic information. The 4 ancillary variables did not contribute to the predictive validity of severe ARDS for mortality and were removed from the definition. Using the Berlin Definition, stages of mild, moderate, and severe ARDS were associated with increased mortality (27%; 95% CI, 24%-30%; 32%; 95% CI, 29%-34%; and 45%; 95% CI, 42%-48%, respectively; P < .001) and increased median duration of mechanical ventilation in survivors (5 days; interquartile [IQR], 2-11; 7 days; IQR, 4-14; and 9 days; IQR, 5-17, respectively; P < .001). Compared with the AECC definition, the final Berlin Definition had better predictive validity for mortality, with an area under the receiver operating curve of 0.577 (95% CI, 0.561-0.593) vs 0.536 (95% CI, 0.520-0.553; P < .001). This updated and revised Berlin Definition for ARDS addresses a number of the limitations of the AECC definition. The approach of combining consensus discussions with empirical evaluation may serve as a model to create more accurate, evidence-based, critical illness syndrome definitions and to better inform clinical care, research, and health services planning.
Ventilator Strategies (ARDSnet.org):
- VT ≦6 mL/kg, Pplat ≦30 cm H2O, allows permissive hypercapnia until maybe pH <7.15. (改善 mortality)
- Titrate PEEP to maintain SaO2 ≧88~90% and (if possible) Pplat ≦30 cm H2O.
- Try to keep FiO2 <0.6 to avoid hyperoxia.